



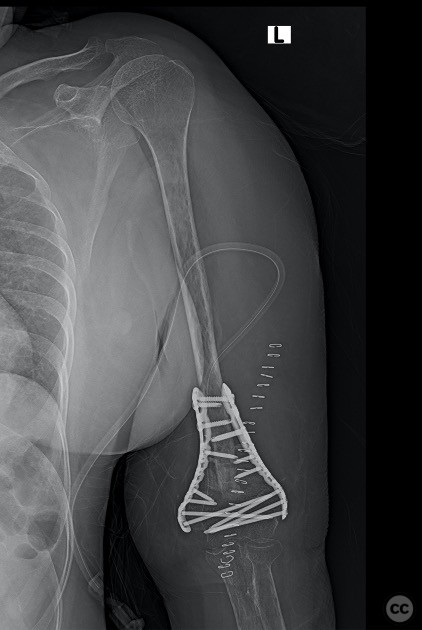



Infected non union of the distal humerus
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: 43-year-old woman with inability to use her left upper limb since 8 months. She was apparently well till 8 months back when she had a fall on out her stretched hand and sustained Isolated closed injury to her elbow. She underwent ORIF and her post operative period was uneventful. On clinical examination the surgical scar healthy, and there were no sinuses. She had stress tenderness at the distal humerus, ROM flexion 20-80 deg with pain and there was no distal neurovascular deficit. Shoulder and wrist -ok. Previous X-rays were not available Investigations: Hb 8.9 GM% Creatinine 0.81 mg% HBA1 C 5.5 % Vitamin D 10 ng/ml ESR 45mm/hr, CRP 6.15 mg/L
Preoperative Plan
Planning remarks: 1stage - removal of implants, radical debridement, 5 deep tissue cultures from the bone implant interface, implants for signification, biopsy , request the microbiologist for extended culture, immobilisation on a above elbow POP slab. Infectious diseases consult for appropriate antimicrobial therapy. To proceed with 2nd stage once the blood markers are normal and after completion of appropriate antimicrobial therapy. 2nd stage- ORIF with autogenous iliac crest bone grafting
Surgical Discussion
Patient positioning: Lateral position
Anatomical surgical approach: Para tricepital approach
Operative remarks:1 st stage - there were signs of infection intraoperatively
2nd stage- acute docking of the non union site, stabilisation with parallel distal humerus anatomically pre contoured LCP and autogenous iliac crest bone grafting.
Postoperative protocol: Post 2nd stage Active elbow ROM exercises
Orthopaedic implants used: Depuy-synthes
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 1388 times
23 Feb 2023
Add to Bookmarks
Full Citation
Cite this article:
Abel. (2023). Infected non union of the distal humerus. Journal of Orthopaedic Surgery and Traumatology. Case Report 10680927 Published Online Feb 23 2023.