






Mason and Molloy 2A Posterior Malleolar Fracture with Posteromedial die punch, and Wagstaffe Fragment
Score and Comment on this Case
Clinical Details
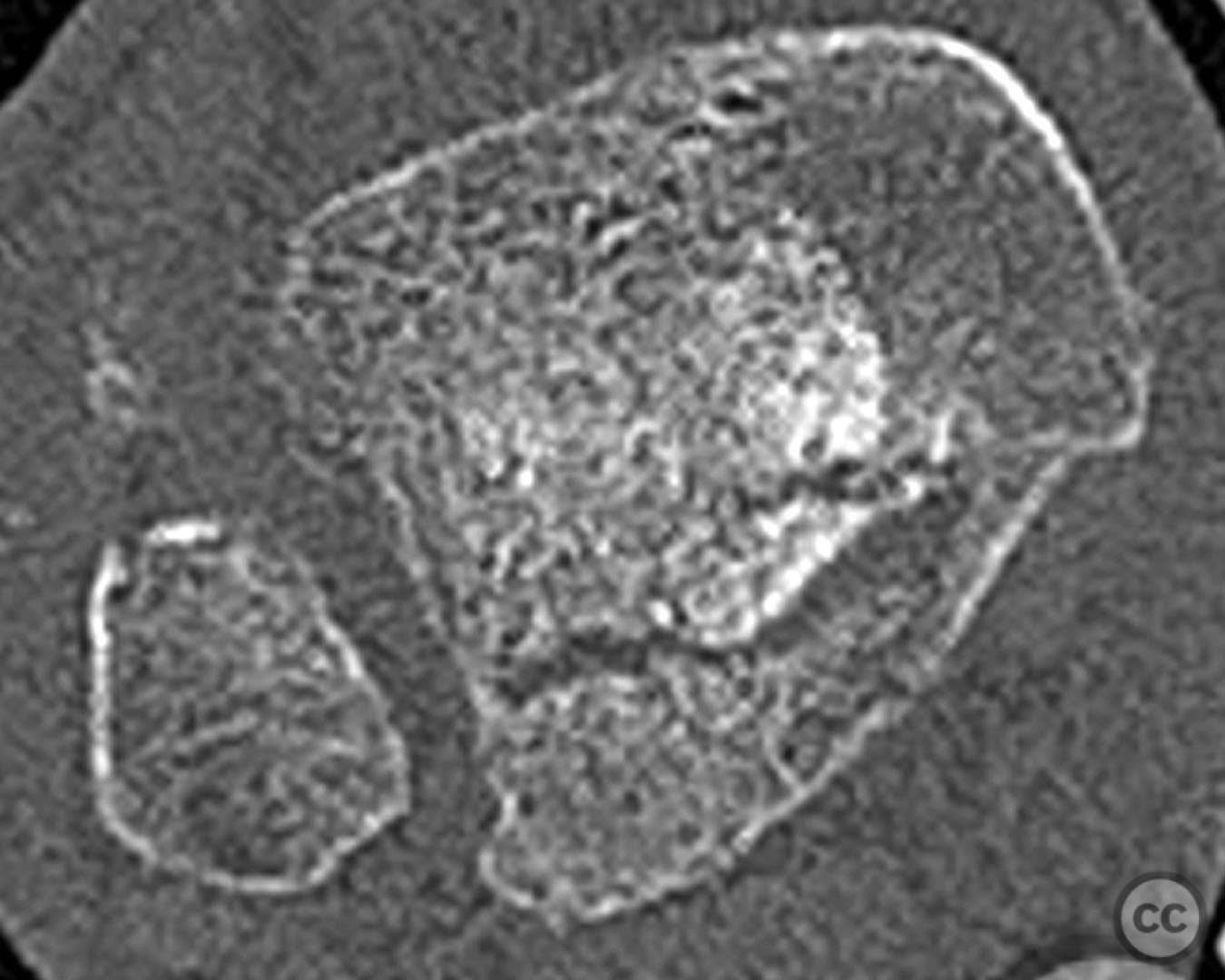
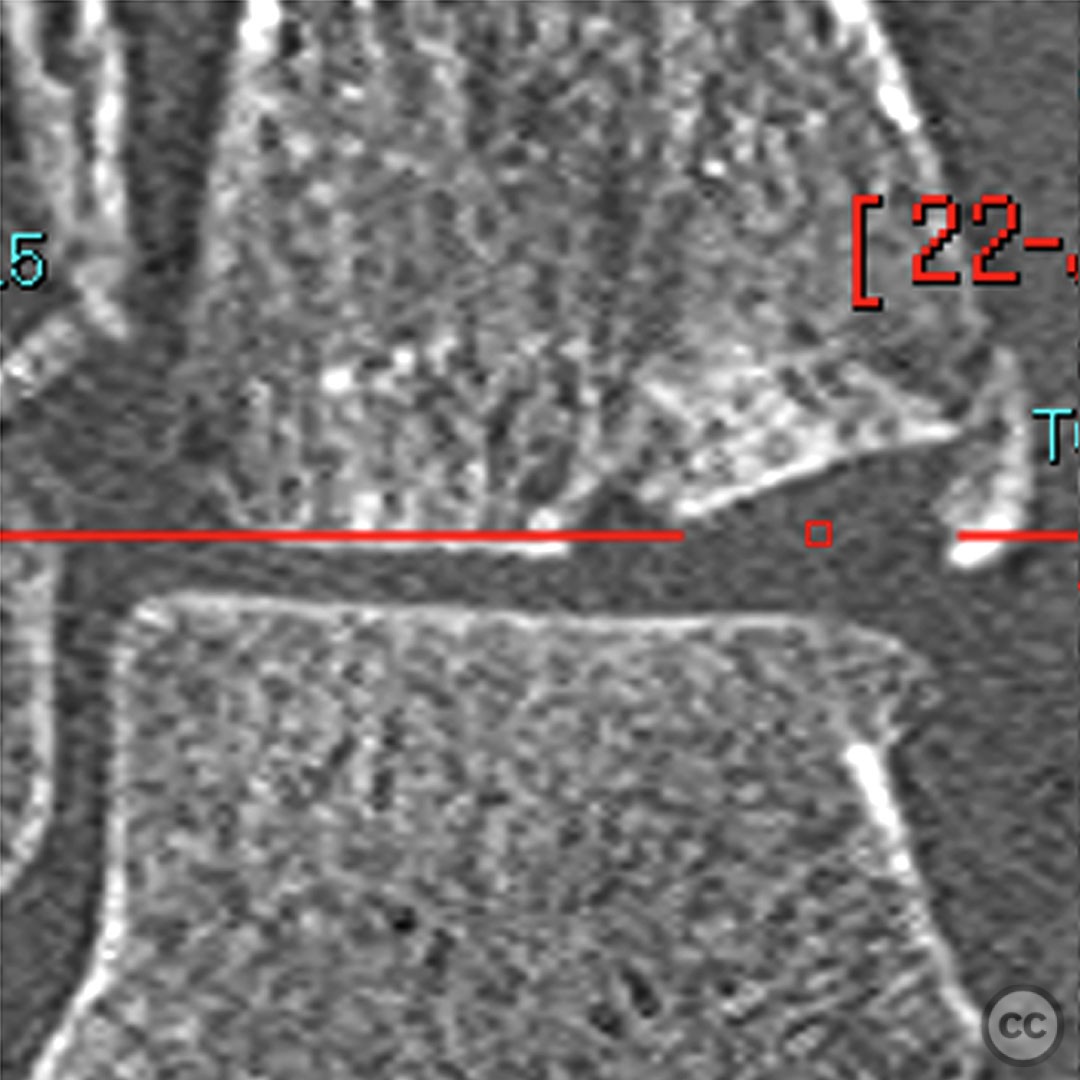
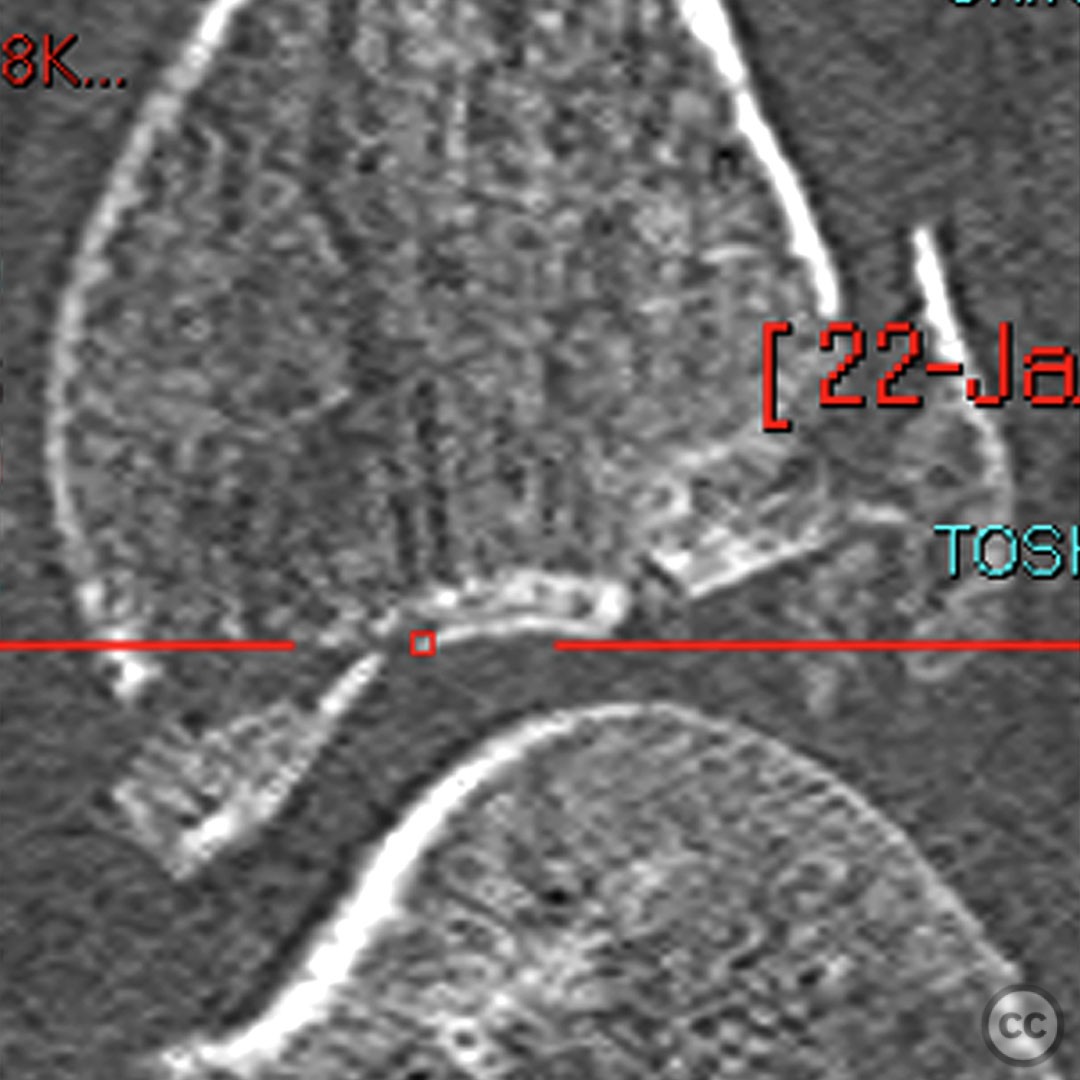
Clinical and radiological findings: Short comminuted fibular fracture, Type 2A PM fracture, anterior collicular fracture. Die punch fragment posteromedial aspect. Avulsion posteromedial of intermalleolar ligament.
Preoperative Plan
Planning remarks: Due to the posteromedial die punch fragment we need to plan access to the die punch. We also need to ensure a comminuted fibular fracture can be accessed and reduced appropriately.
Surgical Discussion
Patient positioning: Recovery position.
Anatomical surgical approach: Lateral and medial posteromedial.
Operative remarks:My approaches were planned to allow confident reduction of the fibular comminution which is more predictable through a direct lateral approach and needing access to the die punch I need to enter through the bed of tibialis posterior. Therefore, a lateral and MPM is easiest in this case. The MPM can be curved anteriorly along the tib post course to allow access the anterior collicular fracture.
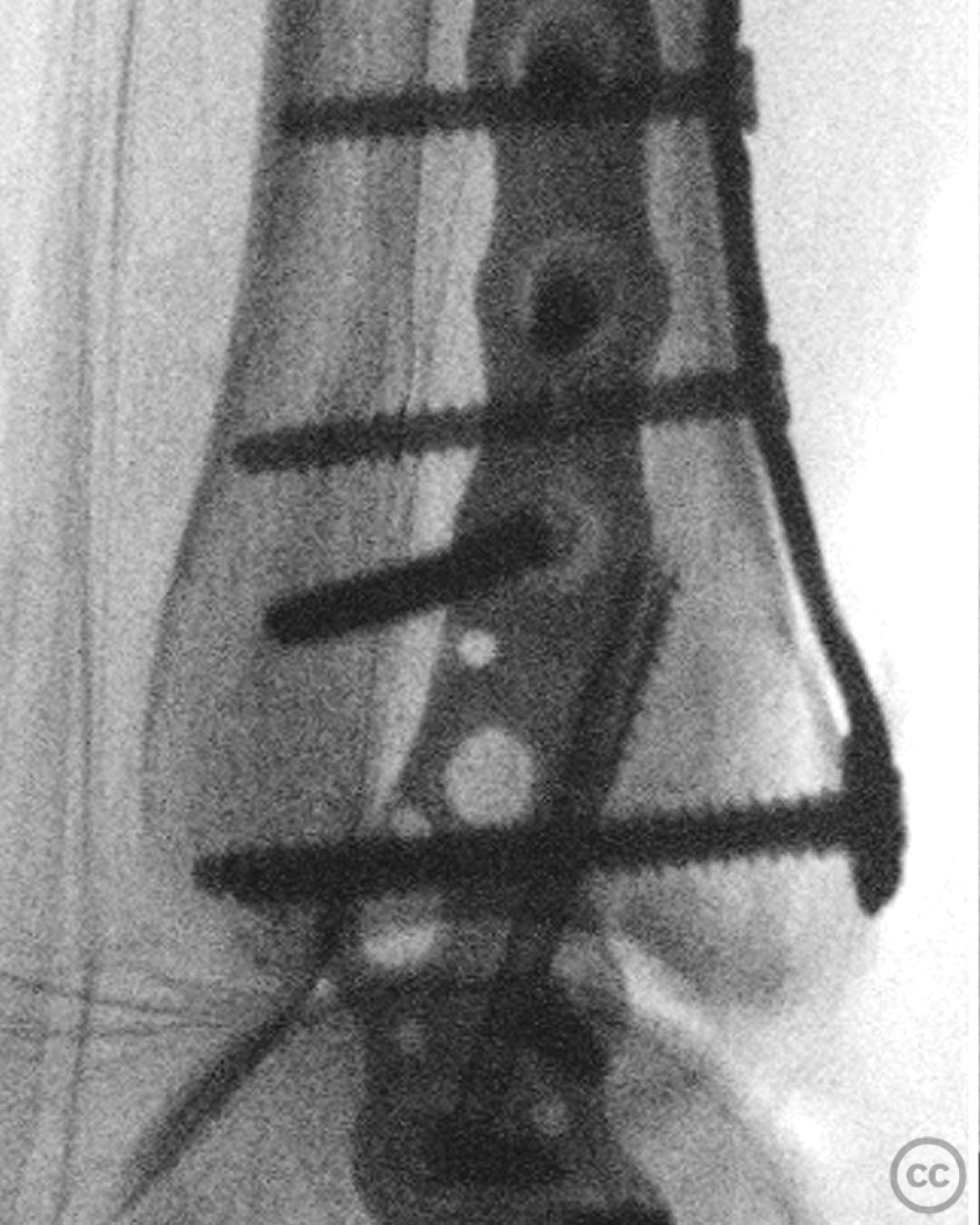
The MPM approach allowed me to open the PL fragment fracture plane to reduce the die punch with a small osteotome. This was K wired in position before application of plate. The PL fragment was then reduced and fixed with a type 3 plate, which fitted best in this case. Note, that the most lateral distal screw is not used as this would encroach on the incisura. The initial buttress screw in the type 3 plate was removed following fibular fixation, to allow syndesmosis fixation.
Postoperative protocol: 2 weeks NWB in a back slab. Conversion to Vacuum cast boot at 2 weeks to allow full weightbearing. Wean out of boot at 6 weeks.
Orthopaedic implants used: Orthosolutions (Volition)
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 811 times
31 Jan 2023
Add to Bookmarks
Full Citation
Cite this article:
Mason, L. (2023). Mason and Molloy 2A Posterior Malleolar Fracture with Posteromedial die punch, and Wagstaffe Fragment. Journal of Orthopaedic Surgery and Traumatology. Case Report 10983394 Published Online Jan 31 2023.