





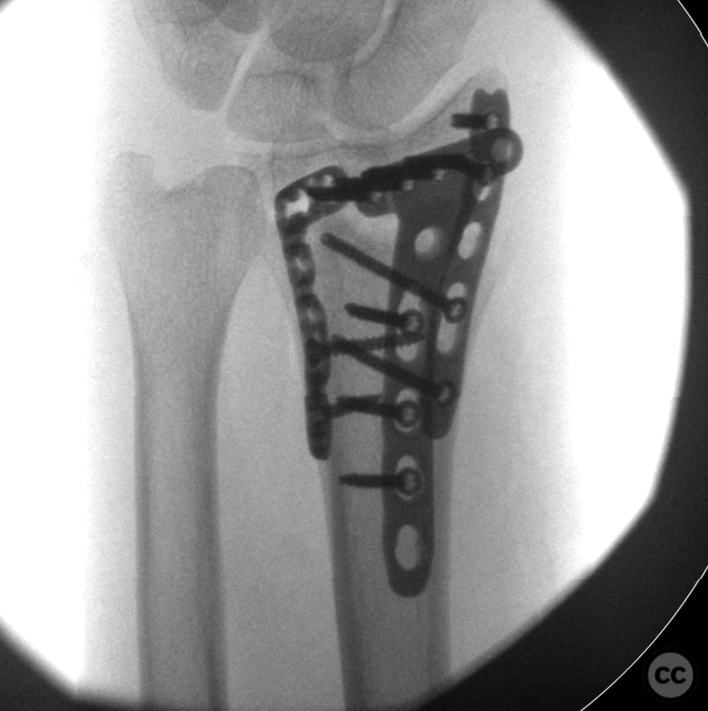
270deg plating of a comminuted distal radius fracture
Score and Comment on this Case
Clinical Details
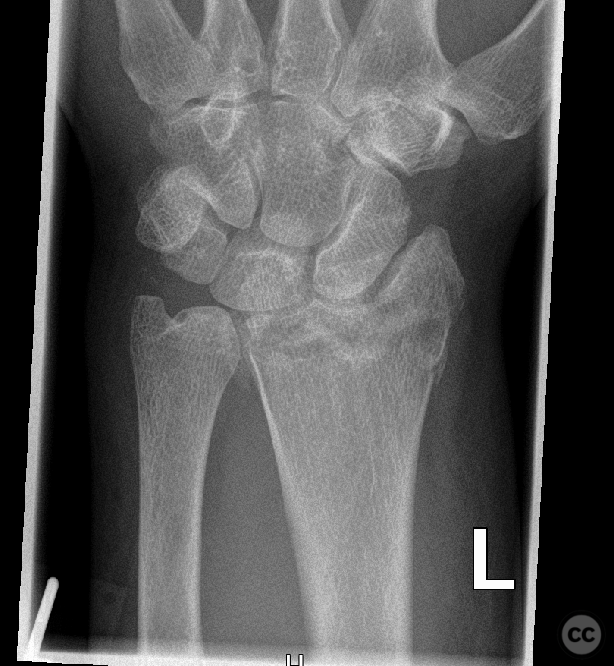
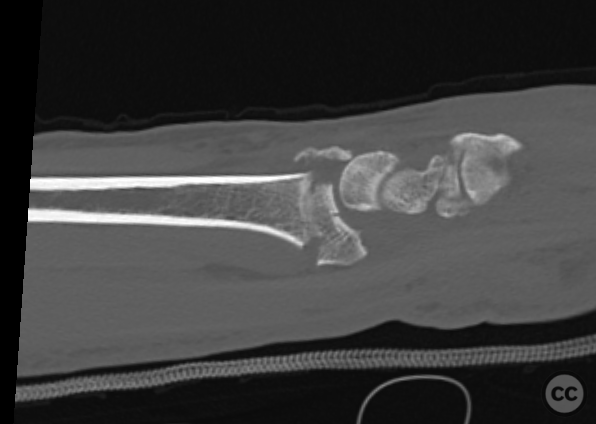
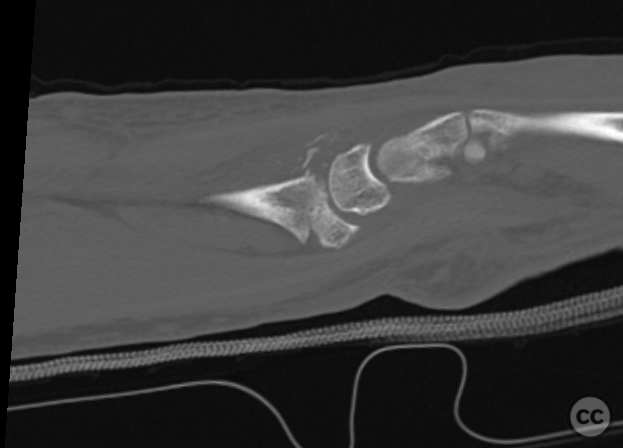
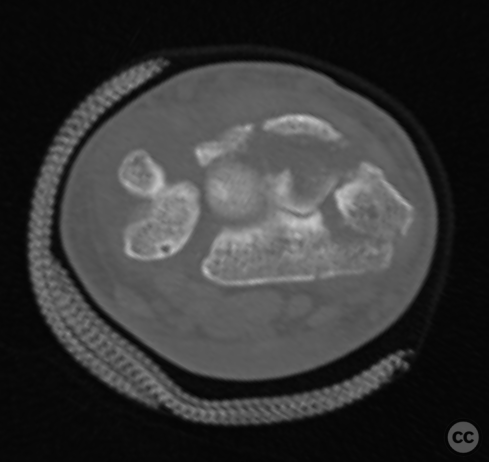
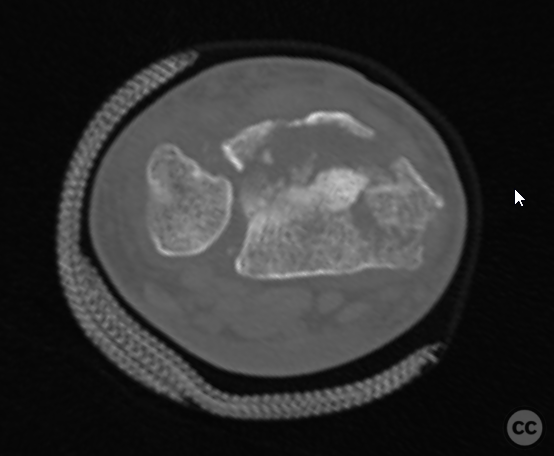
Clinical and radiological findings: This is a 40 year old man following a fall from over 3m onto the outstretched left hand. Closed and neurovascularly intact injury. This injury was immobilized in a splint whilst management of other injuries took priority. Following consolidation of soft tissues operative management took place on the seventh day post injury. As can be seen on CT imaging, there's both volar and dorsal comminution wih subluxation of the carpus. Additionally the radial styloid cmay be appreciated as an independent piece. The volar, intermediate and ulnar column appear intact as an isolated fragment, though the joint surface headed dorsally appears interrupted by some nondisplaced comminuation. The dorsal rim is comprised of a dorsal lunate fragment, and a fragment of listers tubercle. The constellation of these two displaced fragments comprises the dorsal radiocarpal ligament complex, and the dorsal distal radial ulna ligament. This compromises dorsal carpal stability. Additionally the distal radial ulna joint has lost congruity.
Preoperative Plan
Planning remarks:
Surgical Discussion
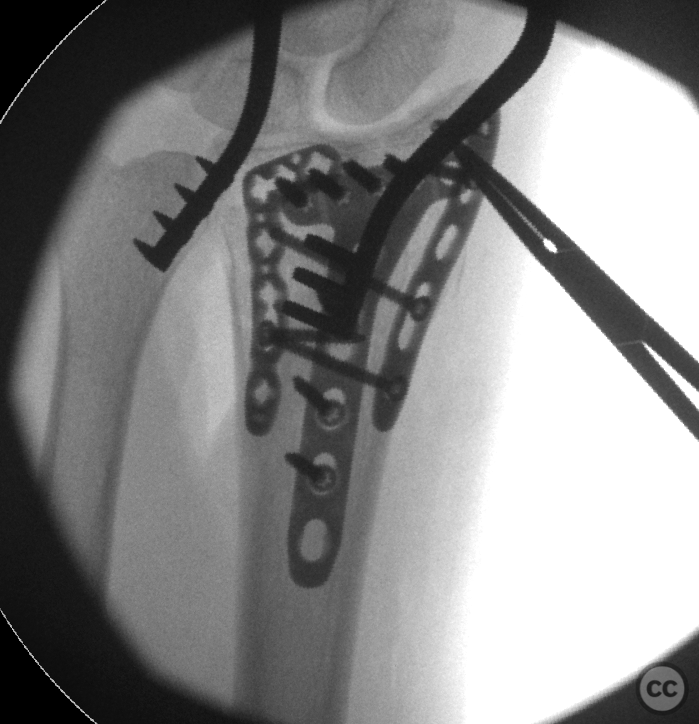
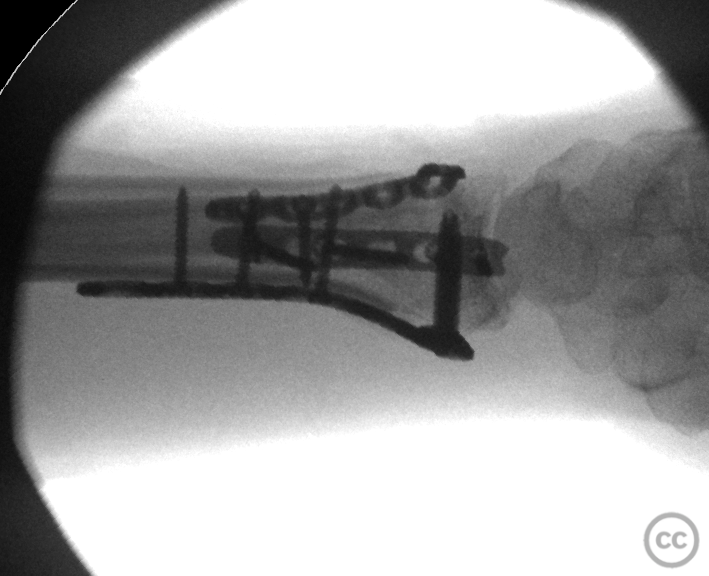
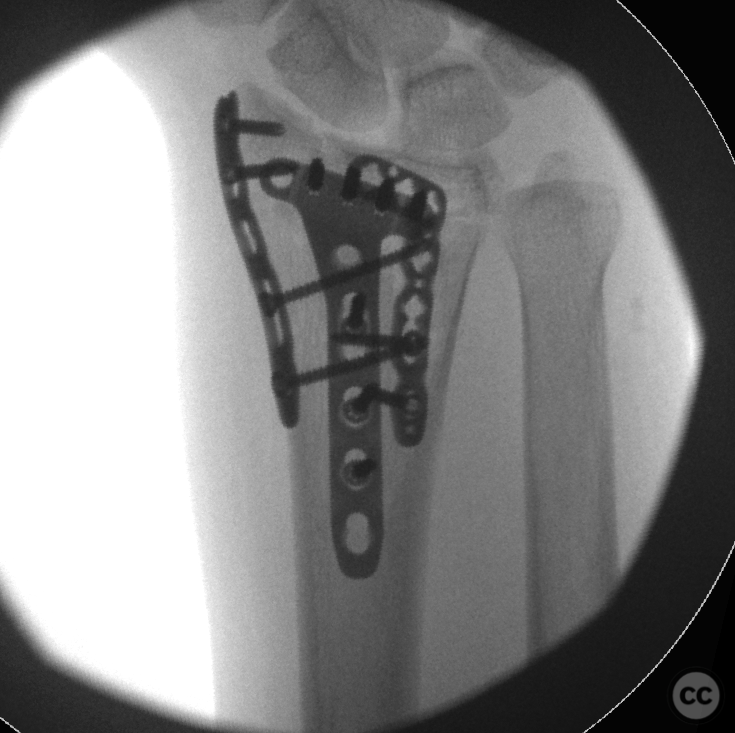
Operative remarks:I figured the easiest place to start would be in reducing the volar intermediate and ulnar columns give this block of intact joint surface could be captured and manipulated as a single unit. This was done with a juxta articular distal radial plate with three subchondral screws, engaging only this fragment piece. The length of the screws was deliberately kept short, so as to not interfere with a secondary dorsal fragment reduction. Reduction of this joint surface fragment was done through positioning of the plate, and reduction of the plate to the distal radial diaphysis achieving neutralization of the dorsal annulation. It became apparent at this point that the radial styloid piece was freely independent, and not reducible in combination with the volar intermediate column. Given real estate limitations on the volar side, fragment specific fixation of the radial styloid through the dorsal approach (together with fixation of the other dorsal fragments) was decided. Incision over the joint centred on Listers. The third extensor compartment was left in tact. Instead, I opened the second compartment to identify the radial styloid fracture and its dorsal aspect. This was reduced and fixed with the k-wire before radial styloid plating along the dorsal radial aspect without opening the first extensor compartment. Then moving to the ulnar side of listers, I open the fourth compartment with EDC/EI and elevated to expose the ulnar aspect of listers fragment, along with the dorsal lunate fragment. These were reduced and fixation was achieved through simple buttress plating without screw fixation. Suture reinforcement of the fragments to the plate through the dorsal capsule and the dorsal radiocarpal ligament along with the distal radioulnar ligament was achieved.
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1525 times
01 Dec 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). 270deg plating of a comminuted distal radius fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 11232315 Published Online Dec 01 2022.