



















Jupiter IIb Monteggia Fracture-Dislocation in a 72-Year-Old
Score and Comment on this Case
Clinical Details
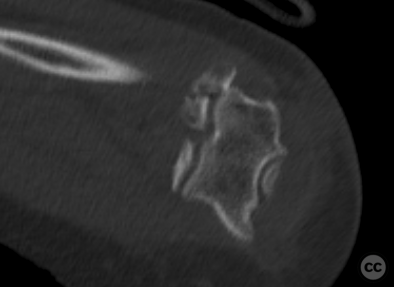
Clinical and radiological findings: A 72-year-old female presented after a domestic fall, sustaining a fracture of the distal radius and a fracture-dislocation of the ipsilateral elbow. Initial radiographs of the elbow revealed a Monteggia type fracture-dislocation with an associated radial head fracture and a Jupiter type IIb proximal ulna fracture. CT scans confirmed these findings and additionally identified a non-displaced large Type I coronoid fracture.
Preoperative Plan
Planning remarks: The preoperative plan included a dorsal approach to both the ulna and radial head. Initial focus was on the coronoid process fracture, planning for fixation with a cannulated Herbert screw. Following this, attention would turn to the proximal ulna fracture, aiming for reduction and stabilization using Kirschner wires facilitating reduction of the radial head dislocation, before addressing the radial head fracture with Herbert screw fixation. Definitive fixation of the ulna fracture was then planned with an anatomical proximal ulna locking plate.
Surgical Discussion
Patient positioning: The patient was positioned supine with the arm positioned in front of the chest, elbow bent at 90 degrees.
Anatomical surgical approach: The surgical approach involved a dorsal incision, utilizing Boyd's interval to separate the anconeus muscle from the ulna. This was followed by sharp division of the lateral ulnar collateral ligament (LUCL) from the supinator ridge to access the proximal radioulnar joint (PRUJ) and radial head, while also allowing visualization of the coronoid process. A limited Taylor-Sham approach was used ulnarly to assess and reduce the ulna fracture.
Operative remarks:Initially, the non-displaced coronoid fragment was secured with a cannulated Herbert screw prior to the manipulation of any other fractures. Subsequently, the PUDA was reduced and held using K-wires. This resulted in concomitant reduction of the radial head dislocation allowing fixation of the radial head fragments using HBS screws in both a fragment-specific and strut-construct arrrangement. The definitive fixation of the ulna fracture was achieved with an anatomical proximal ulna locking plate. Passive range of motion (PROM) was tested intraoperatively under fluoroscopy, confirming no instability through the full range of motion.
Postoperative protocol: Postoperatively, no splint was applied, and full active/passive range of motion (A/PROM) was encouraged immediately.
Follow up: Not specified.
Orthopaedic implants used: Cannulated Herbert screw, Kirschner wires, Headless Compression Screws (HBS), Anatomical Proximal Ulna Locking Plate.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 867 times
07 Mar 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Jupiter IIb Monteggia Fracture-Dislocation in a 72-Year-Old. Journal of Orthopaedic Surgery and Traumatology. Case Report 14101588 Published Online Mar 07 2024.