







Subactue posterolateral elbow instability - LUCL internal brace stabilisation
Score and Comment on this Case
Clinical Details
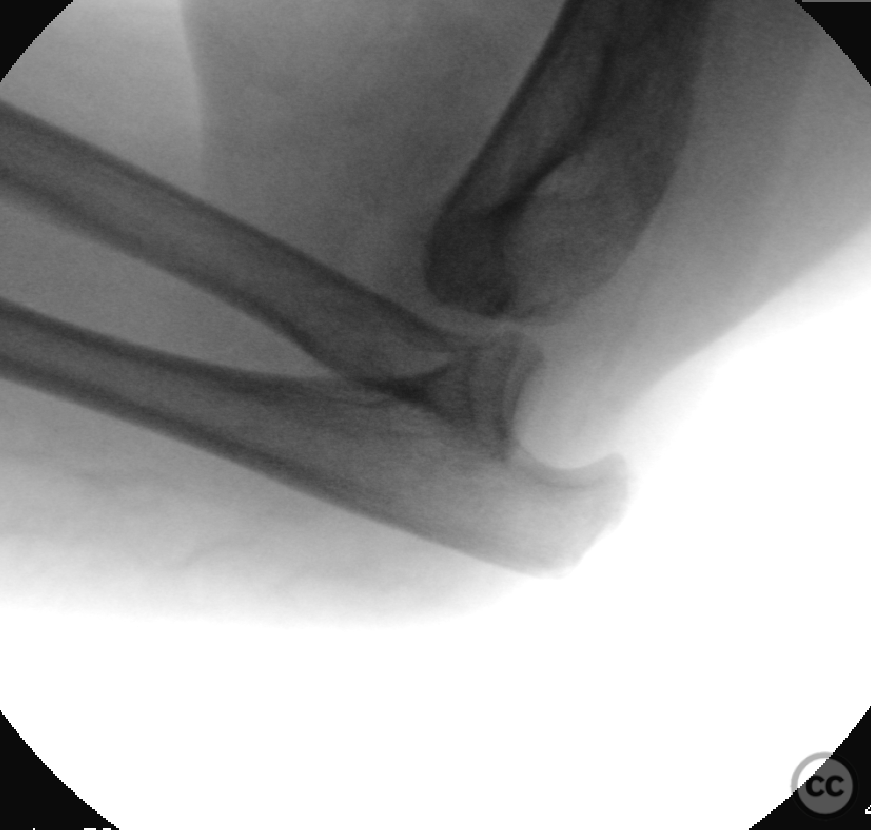
Clinical and radiological findings: Traumatic posterolateral simple elbow dislocation in a 60yo obese patient with poor muscle mass. Initially reduced and immobilsed in a long arm cast in ER. Patient subsequently lost to followup finally representing 5 weeks post injury with a malpositioned cast and the elbow posterolaterally dislocated in the cast. Duration of dislocation can be assumed to be at least several weeks. Closed injury. NV intact.
Preoperative Plan
Planning remarks:
Surgical Discussion
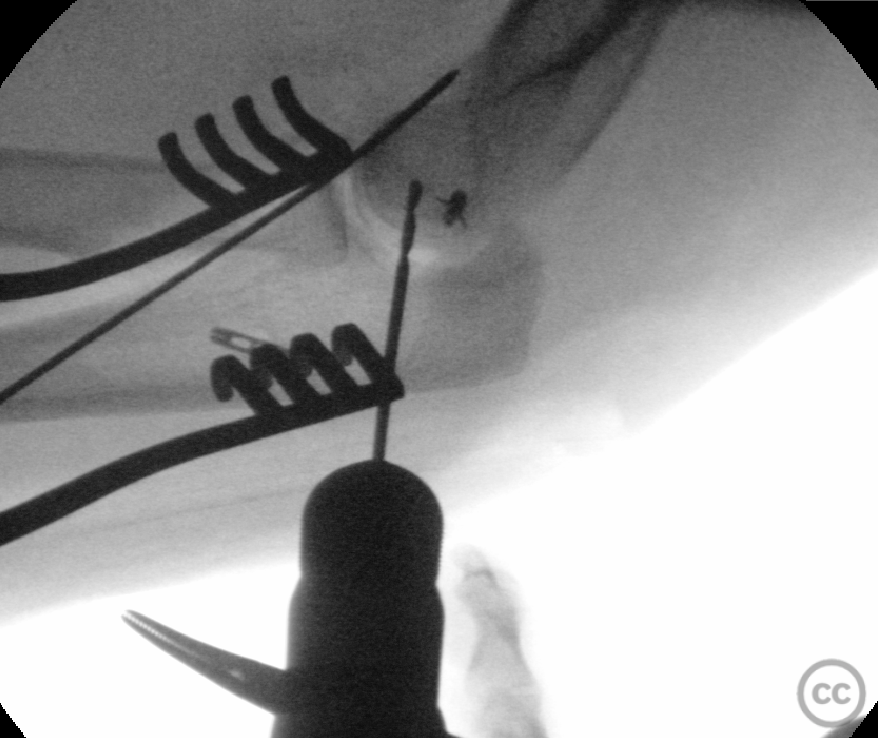
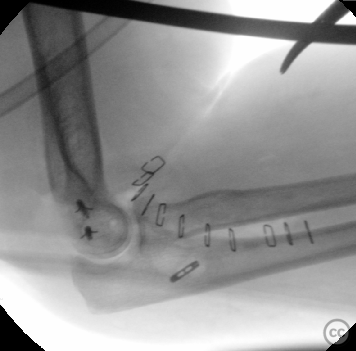
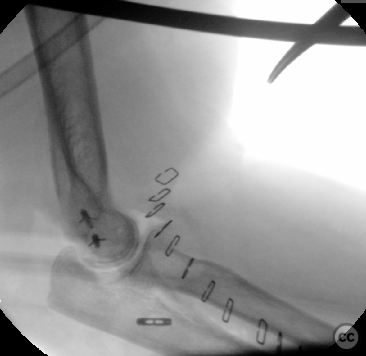
Operative remarks:Supine position, arm on an positional arm support. Initial fluro images show incongruent reduction and instability at even 80-90deg. Started laterally - Kocher approach. LCL common origin found avulsed from the capitellum with early pannus tissue. Ligamental structures a bit mushy. Dercided early to augment repair with an internal brace. Endobutton armed with #2 fibertape brought into the lateral ulna just inferior and distal to LUCL insertion on the supinator crest. GII Anker fixation of the common LCL origin just posterior to the isometric point on the capitellum which was reserved for a pushlock anchor. Isometric point on the lateral capitellum was drilled 2.0mm (see image) and 2.9mm Pushlock anchor with #2 Suturetape was provisionally inserted and tested. Dynamic ROM confirmed stable isometrics. Lateral stabilisation achieved joint stability and congruency through a PROM to 50deg extension before humeroulnar subluxation occured. Valgus stress identified gross medial gapping. Repositioning of the arm and FCU split approach to the ulnar nerve and medial epicondyle. Complete avulsion of humeral MCL origin was evident, the ligamental substance was medially structurally sound. Anatomical non isometric GII anchor fixation of the MCL origin in 60deg. Dynamic ROM under fluroscopy demonstrated congruent stability to 40deg extension with restored physiological valgus stress gapping. Joint stiffness was encountered at 30-40deg due to previous cast immobilisation. With this extension block mild incongruity and subluxation of the humeroulnar joint began at 30deg (last image). Given congruity to +40deg a we decided to desist with further medial reconstruction and will encourgae post op rehabilitation in a ROM brace blocked at 40deg for 4 weeks, then 20deg for 2 weeks, the 0deg for a further 2 weeks.
Orthopaedic implants used: Arthrex biceps endobutton, #2 Fibersture, 2.9mm Pushlock anchor (LUCL internal brace), and 2 DePuy Mitek GII anchors (LCL and MCL refixation)
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1335 times
23 Nov 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Subactue posterolateral elbow instability - LUCL internal brace stabilisation. Journal of Orthopaedic Surgery and Traumatology. Case Report 17137959 Published Online Nov 23 2022.