










Distal Radius Fracture with Flipped Die-Punch Fragment
Score and Comment on this Case
Clinical Details
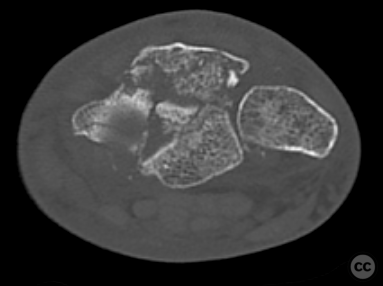
Clinical and radiological findings: A 67-year-old male presented after sustaining a distal radius fracture approximately three weeks prior while on holiday. Initial management at a local hospital involved immobilization in a plaster cast. Upon return, an external local trauma center attempted closed reduction and application of an external fixator. Postoperative CT demonstrated poor reduction with a central die-punch fragment flipped 180 degrees and wedged in the scapholunate joint. The decision was made to proceed with open reduction and internal fixation to achieve better joint reconstruction.
Preoperative Plan
Planning remarks: The planned surgical approach was an extenden volar approach (EFCR) to the distal radius via a longitudinal incision over the flexor carpi radialis tendon to the trapezium. The goal was to achieve anatomical reduction of the flipped die-punch fragment and stabilize the fracture with a volar plate.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table, with the right arm placed on an axillary arm table. A pneumatic tourniquet was applied to the proximal arm.
Anatomical surgical approach: A longitudinal incision was made over the flexor carpi radialis tendon, extending in a radial-sided zigzag fashion over the flexor crease. Subcutaneous hemostasis was achieved, and the flexor carpi radialis tendon was identified and released from its attachment on the radial side of the trapezium. The antebrachial fascia was incised, and the flexor pollicis longus muscle and tendon were retracted ulnarly. A sharp incision along the radial border of the pronator quadratus muscle was made, reflecting it ulnarly to expose the distal radius. Axial traction was achieved through ligamentotaxis on the Scaphoid, and a pronation of the radial shaft allowed semicircumfrential debridement of callus formation
Operative remarks:The central die-punch fragment was identified, removed, and turned around to reconstruct its articular surface accurately before being repositioned. Provisional fixation was achieved using 1.2-millimeter K-wires. A 3+7 millimeter two-column volar distal radius plate was placed and fixed with a single bicortical 2.4-millimeter screw in its shaft portion. Under fluoroscopic guidance, five subchondral screws were introduced into the articular surface, engaging dorsal fragments appropriately. Two additional bicortical 2.4-millimeter screws were placed proximally in the plate. Multiplanar fluoroscopy confirmed proper restoration of joint geometry and articular surface without intra-articular screw penetration or dorsal screw perforation into extensor tendon compartments.
Postoperative protocol: Postoperative rehabilitation involved no splinting during the day, with early mobilization encouraged.
Follow up: Not specified
Orthopaedic implants used: Orthopaedic implants used: - 1.8-millimeter Kirschner wires - 1.2-millimeter Kirschner wires - 3+7 hole two-column volar distal radius plate (Synthes)
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 2147 times
03 Jun 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Distal Radius Fracture with Flipped Die-Punch Fragment. Journal of Orthopaedic Surgery and Traumatology. Case Report 1733387 Published Online Jun 03 2024.