












Dubberly 3/4 shear plus comminuted trans condylar trochlear fracture distal humerus
Score and Comment on this Case
Clinical Details
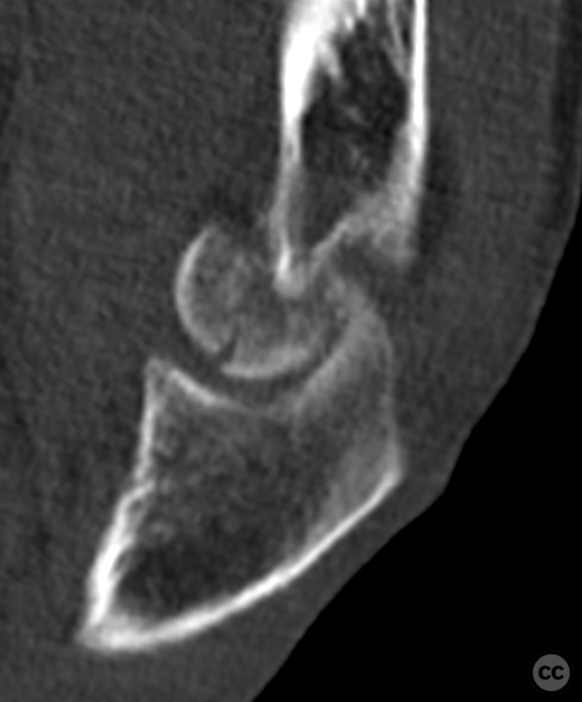
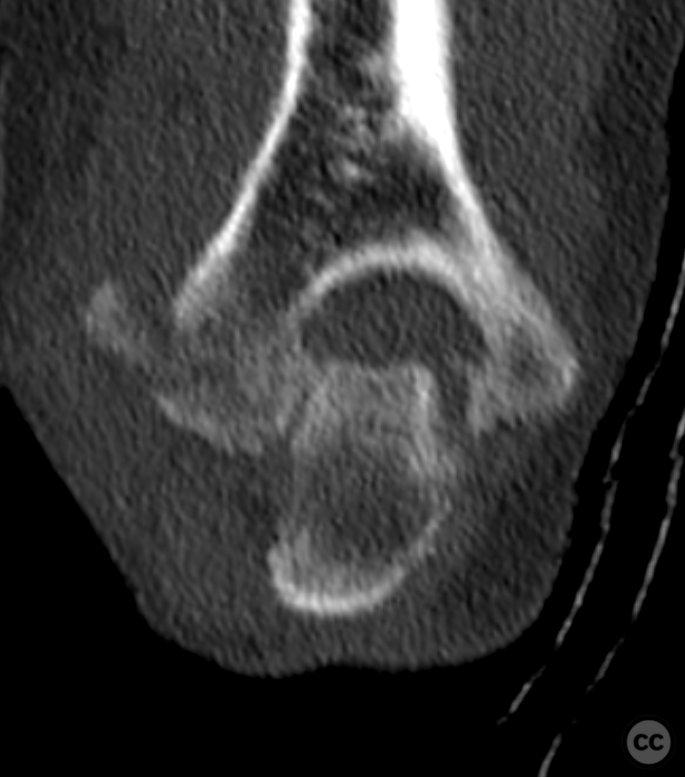
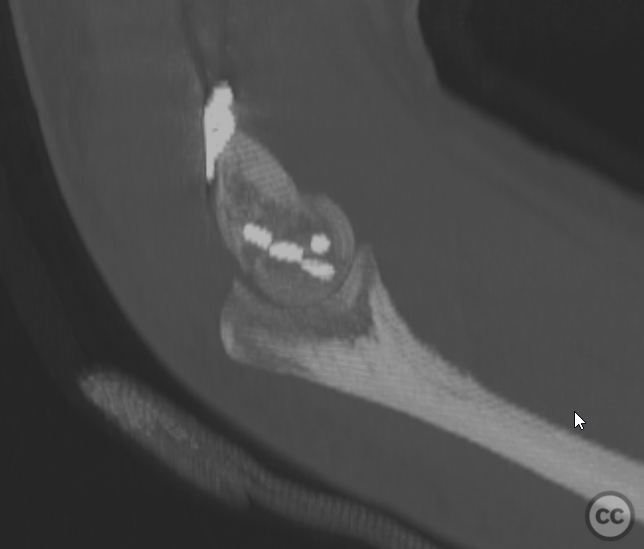
Clinical and radiological findings: This is a highly active 65 year old female who sustained a low energy household fall. A closed and neurovascularly intact isolated injury of the upper limb. As common with these injuries plain film imaging does not necessarily demonstrate the complexity of the injury. The true extent is appreciated on CT in particular in the individual cross sections. This is what is best described as a Dubberly type 4 injury - an extension of the the classical Dubberly classification system as proposed by Joideep Phandis (see linked article below). Essentially this is a multi fragmentary shear injury of both capitellar and trochlear articular surfaces with comminuted dorsal extension into both columns. These injuries are very hard to reconstruct and the incidence of conversion to arthroplasty is high. Given the patient's age and level of activity an attempt at at joint-conserving reconstruction was decided.
Preoperative Plan
Planning remarks:
Surgical Discussion
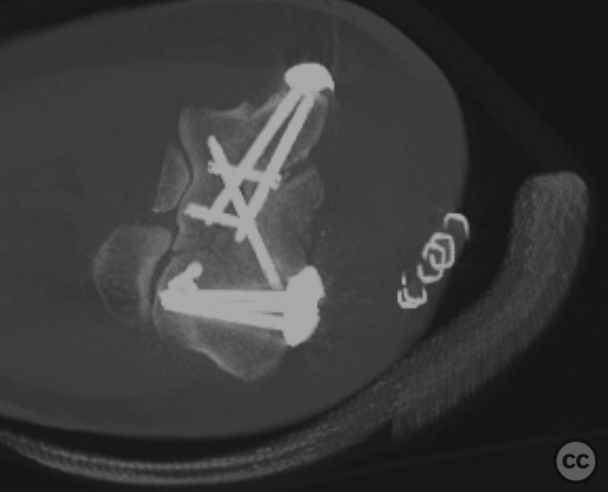
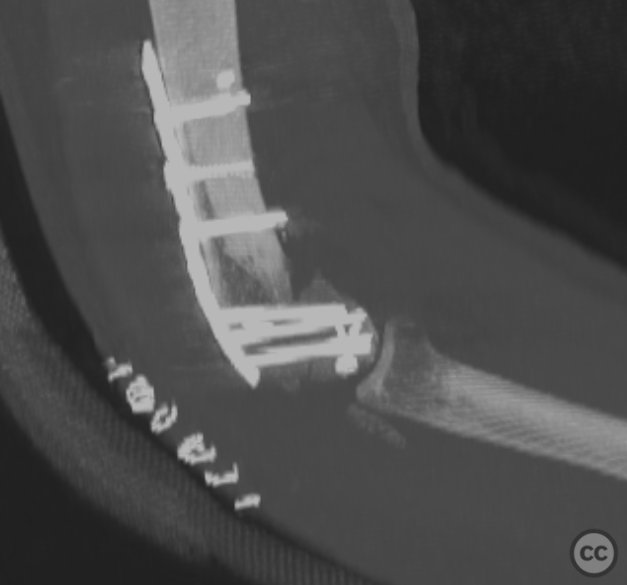
Operative remarks:This case was done supine with the arm freely draped, the elbow flexed to 90 degrees with the forearm held by an arm support placed in front of the patients chest. A combination approach of medial paratricipital and lateral paraolecanon was used. Due to to radial involvement of the lateral collateral origin a medial subluxation of the the ulna was possible allowing access for articular reconstruction without osteotomy. A slow and tedious reconstruction of multiple fragments followed with use of absorbable k wires and headless bone screws recreating an articular block. this block was then reconstructed to to the distal humerus and fixed with 90-degree plating. Intraoperatively this construct was stable and offered a free range of motion 0-20-120 degrees. A postoperative CT scan was performed to confirm quality of reduction. Some proximalisation of the jointline axis in the coronal plane may be appreciated however reconstruction of joint congruity is excellent. Clinical follow-up at 6 weeks together with a follow-up CT scan demonstrated unchanged reduction and maintenance of all hardware. unfortunately clinical range of motion had deteriorated to 0-40-50 degrees representing a functional arc only 10 degrees motion. An intensive physiotherapy rehab regime was instituted at this point. Further follow-up is pending
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 966 times
08 Nov 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Dubberly 3/4 shear plus comminuted trans condylar trochlear fracture distal humerus. Journal of Orthopaedic Surgery and Traumatology. Case Report 18878599 Published Online Nov 08 2022.