



Nonunion of Humeral Diaphyseal Fracture Treated with Locked Plating and Iliac Crest Graft.
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 68-year-old female presented with an 8-month history of nonunion of a diaphyseal humeral fracture. The fracture had been initially managed conservatively using the Sarmiento technique. Radiographic evaluation confirmed the presence of nonunion, with no evidence of callus formation or bridging trabeculae across the fracture site. Neurovascular examination was unremarkable.
Preoperative Plan
Planning remarks: The preoperative plan involved performing an open reduction and internal fixation using a proximal humerus locking plate. The approach selected was an extended deltopectoral incision to allow adequate exposure for fracture site debridement and exploration of the radial nerve. High-strength suture cerclage would be employed to provide additional stability, and autologous bone grafting from the iliac crest was planned to enhance osteogenesis at the nonunion site.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table, with the arm placed on a radiolucent arm board to facilitate intraoperative imaging and manipulation.
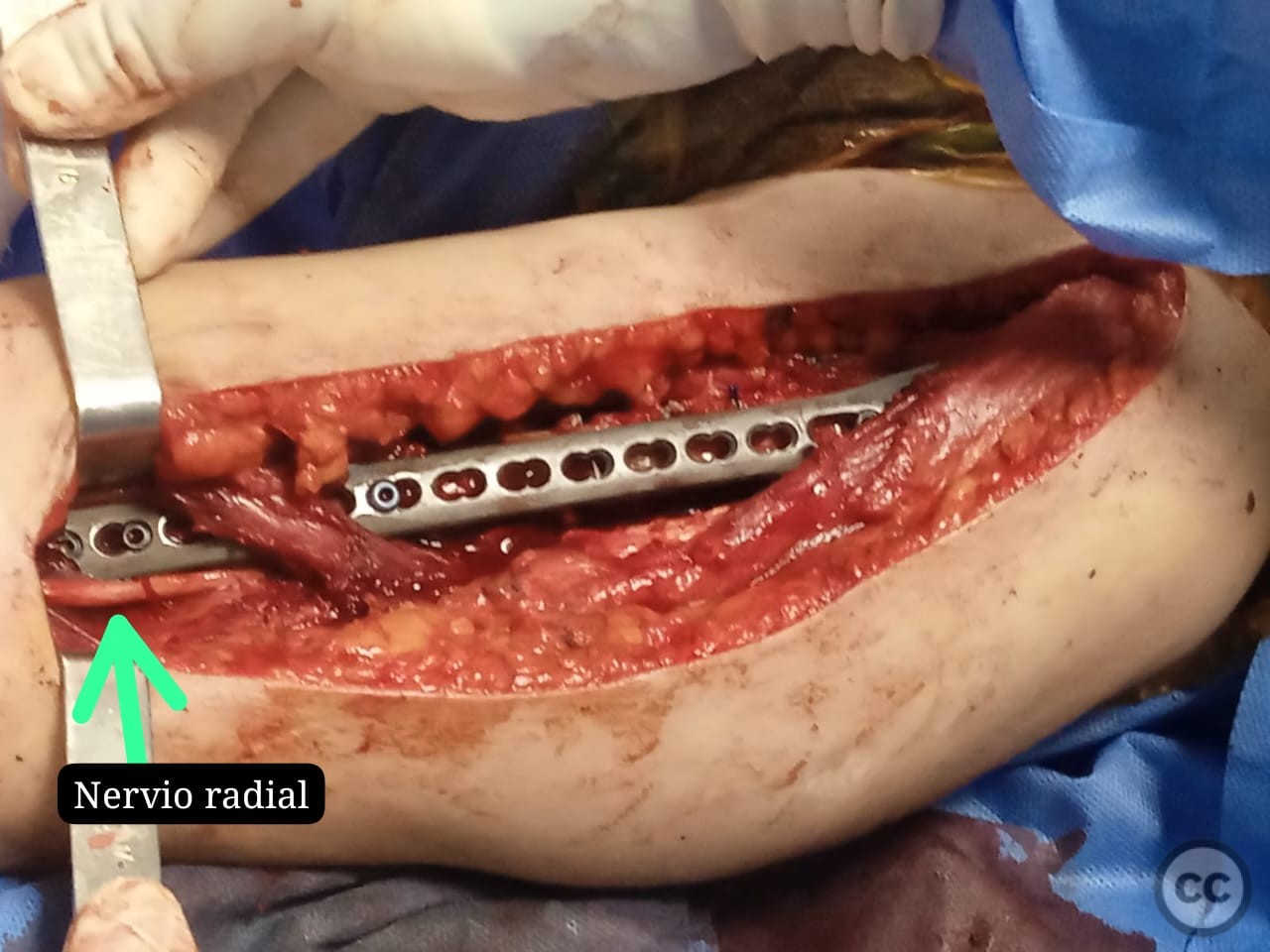
Anatomical surgical approach: An extended deltopectoral approach was utilized, beginning at the coracoid process and extending distally along the deltopectoral groove. The cephalic vein was identified and retracted laterally. Subperiosteal dissection was performed to expose the humeral shaft. The fracture site was debrided, and the radial nerve was carefully identified and protected throughout the procedure.
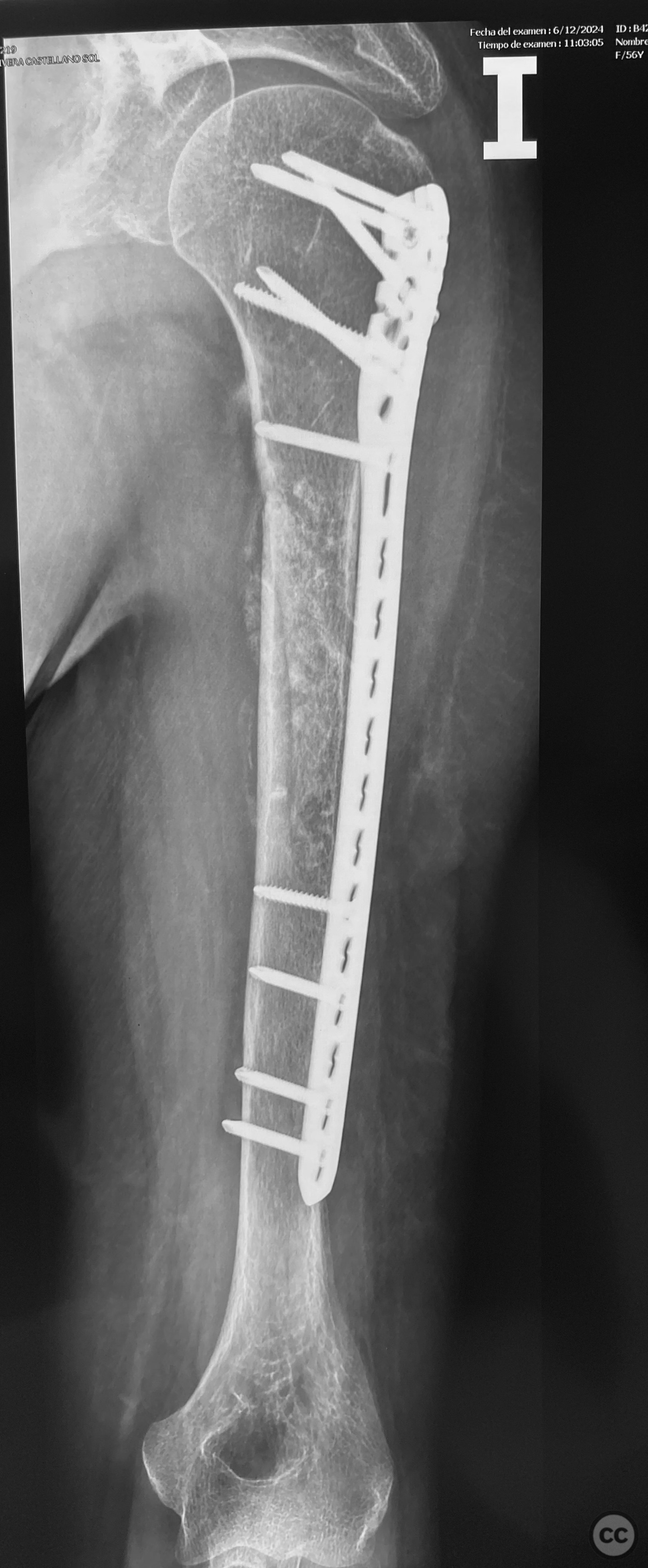
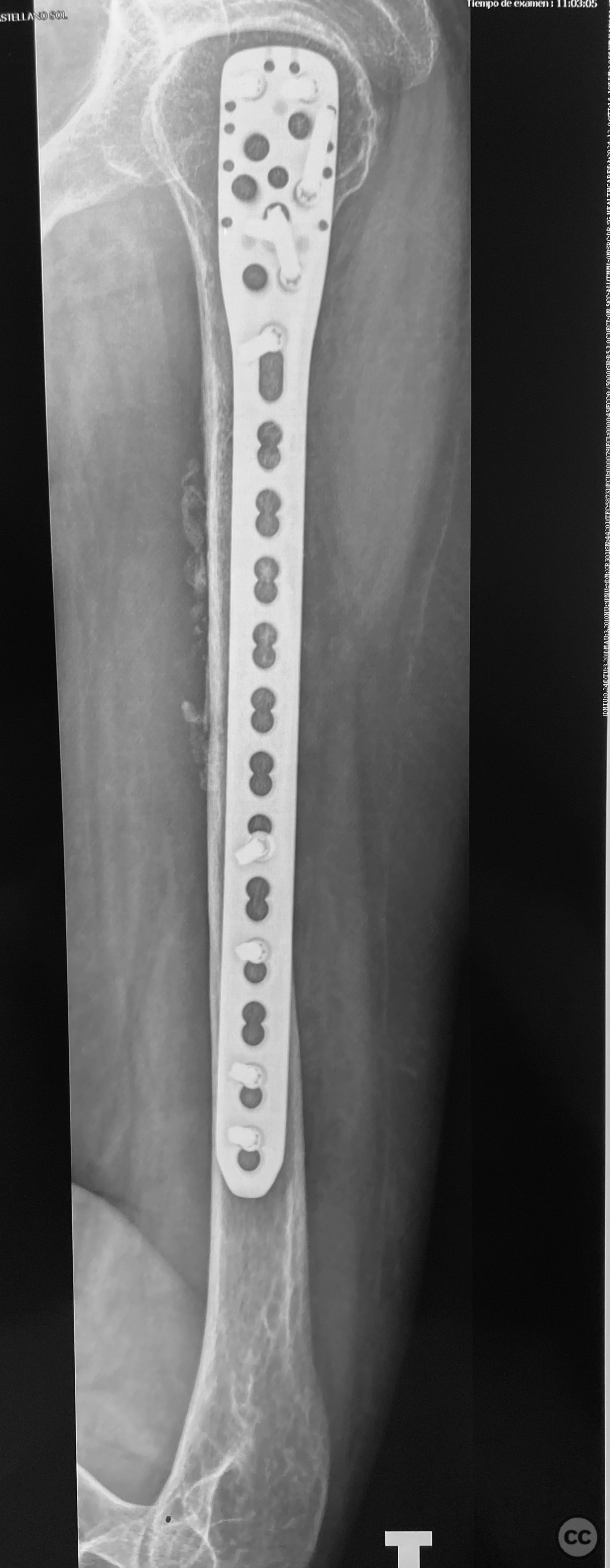
Operative remarks:The fracture edges were refreshed to promote healing. Three cerclages using high-strength suture with Niza knot technique were applied for provisional stabilization. The radial nerve was explored and protected during the procedure. A proximal humerus locking plate was then applied for definitive fixation. Autologous bone graft harvested from the iliac crest was placed at the nonunion site to facilitate bone healing.
Postoperative protocol: Postoperatively, the patient was advised to wear a sling for comfort. Passive range of motion exercises were initiated immediately, with active-assisted exercises introduced at 2 weeks post-surgery. Weight-bearing activities were restricted until radiographic evidence of union was observed.
Follow up: Not specified.
Orthopaedic implants used: Proximal humerus locking plate, high-strength suture cerclage (Nudo Niza), iliac crest bone graft.
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 430 times
30 Dec 2024
Add to Bookmarks
Full Citation
Cite this article:
LUIS LEONCIO TEMOCHE DIAZ. (2024). Nonunion of Humeral Diaphyseal Fracture Treated with Locked Plating and Iliac Crest Graft.. Journal of Orthopaedic Surgery and Traumatology. Case Report 19621085 Published Online Dec 30 2024.