
.png)

.png)
.png)
.png)

.png)

.png)
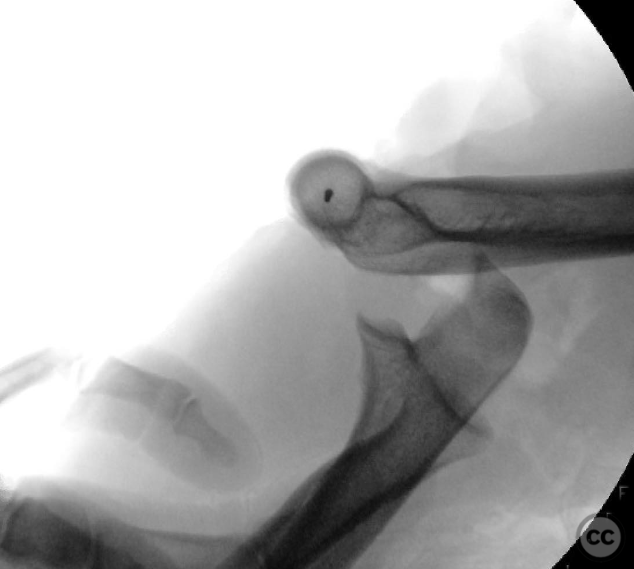
Internal Joint Stabilizer IJS® open posterior elbow dislocation
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: This was an open (obviously) posterior elbow dislocation. She presented with a banged up but perfused (mostly) hand. Neuro exam challenging on presentation. She was brought urgently to the OR by my partner for debridement , irrigation and exploration. All major nerves about the elbow in continuity, no arterial injury. Massively contaminated. She underwent a very thorough debridement (several hours of trimming, picking, washing, scratching, etc to decontaminate) and then splinting. I took her back 48hr later for a second look.
Preoperative Plan
Planning remarks:
Surgical Discussion
Operative remarks:Brachialis smoked, capsule smoked, MUCL not repairable. Basically the only soft tissue structure intact was triceps. I made a kocher approach and found (as is typical) the LUCL and common extensor origin off the lateral epicondyle and repairable. Given the global instability and inability to repair medial structures I elected for 1) reduction 2) LUCL and CEO repair 3) internal ex-fix. Historically we would do 1 and 2 and then a static or hinged ex-fix. Hinged ex fixes were basically a disaster. Static ex fixes suck because you are guaranteed a super stiff elbow. The benefit of the internal ex fix is augmented stability and motion(as the soft tissues allow). The soft tissue injury was treated with primary closure and STSG. The in fix comes out between 3 and 6 months. I’ve seen this thing used with increasing frequency over the last few years for injuries that are otherwise repairable with early motion allowed. It’s not an off the shelf device for terrible triads and other variations of simple ligamentous injuries. But when you need it, it’s a good tool.
Orthopaedic implants used: Skeletal Dynamics - IJS
Author's Resources & References
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1028 times
15 Jan 2023
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2023). Internal Joint Stabilizer IJS® open posterior elbow dislocation. Journal of Orthopaedic Surgery and Traumatology. Case Report 19723207 Published Online Jan 15 2023.