





C3 distal humerus with olecranon osteotomy
Score and Comment on this Case
Clinical Details
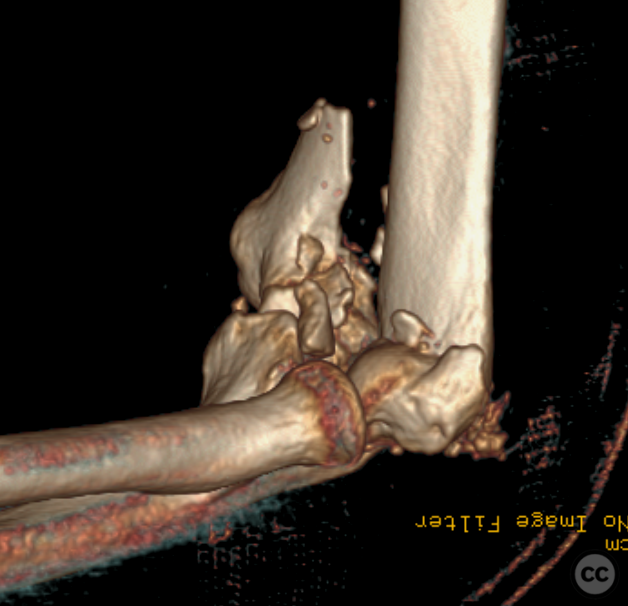
Clinical and radiological findings: This cases of a 70-year old alcoholic following an intoxicated full who sustained the above comminuted distal humerus fracture. A closed injury the arm was neurovascularly intact. Plain film imaging is not provided as as only CT imaging can truly demonstrate the extent of injury. Here is a sagittal split of the ulnar column evident with a sagittal split separating trochlea from capitellum. There are multiple small comminuted fragments inbetween these main fragments. Also dorsally in the transition to the olecranon fossa several trochlea fragments are evident. The history suggested that this was a fresh fracture. However the reliability of the patient came into question intraoperatively as as a blunted rounding of the fragments along with callous interposition would suggest a fracture several weeks old. The pre-operative plan did not predict the need for an osteotomy however after initial intra-operative assessment this plan was modified
Preoperative Plan
Planning remarks:
Surgical Discussion
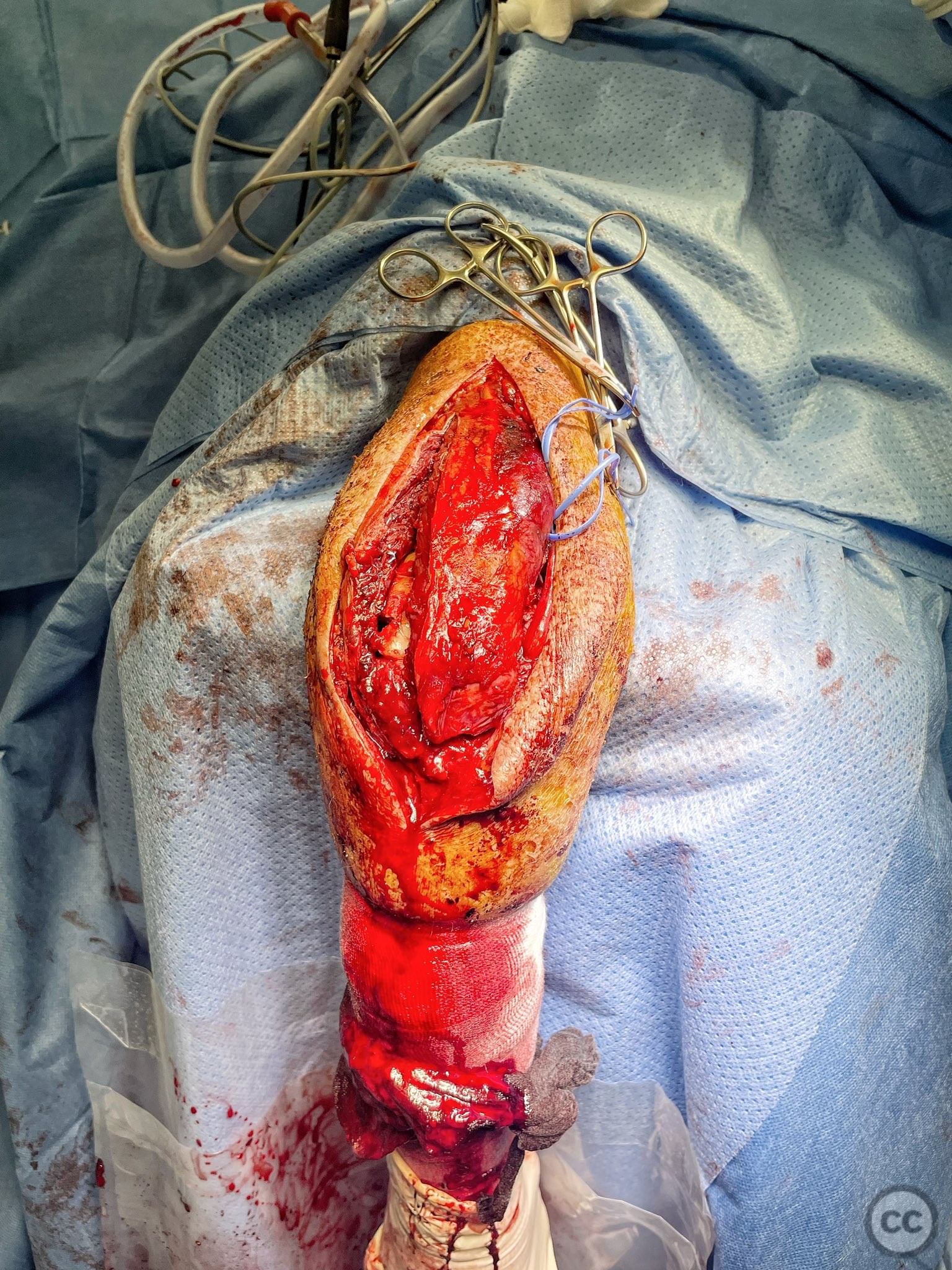
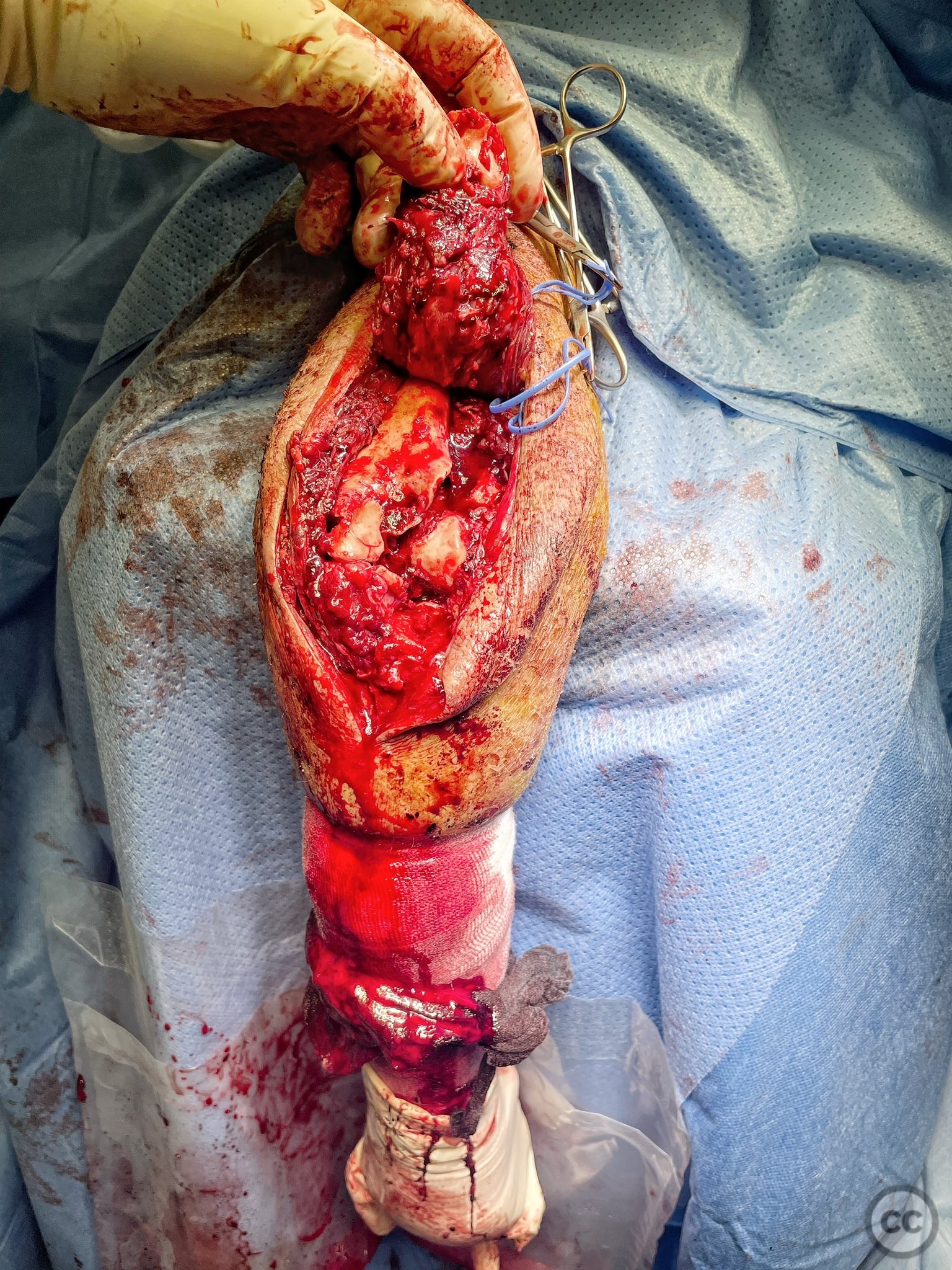
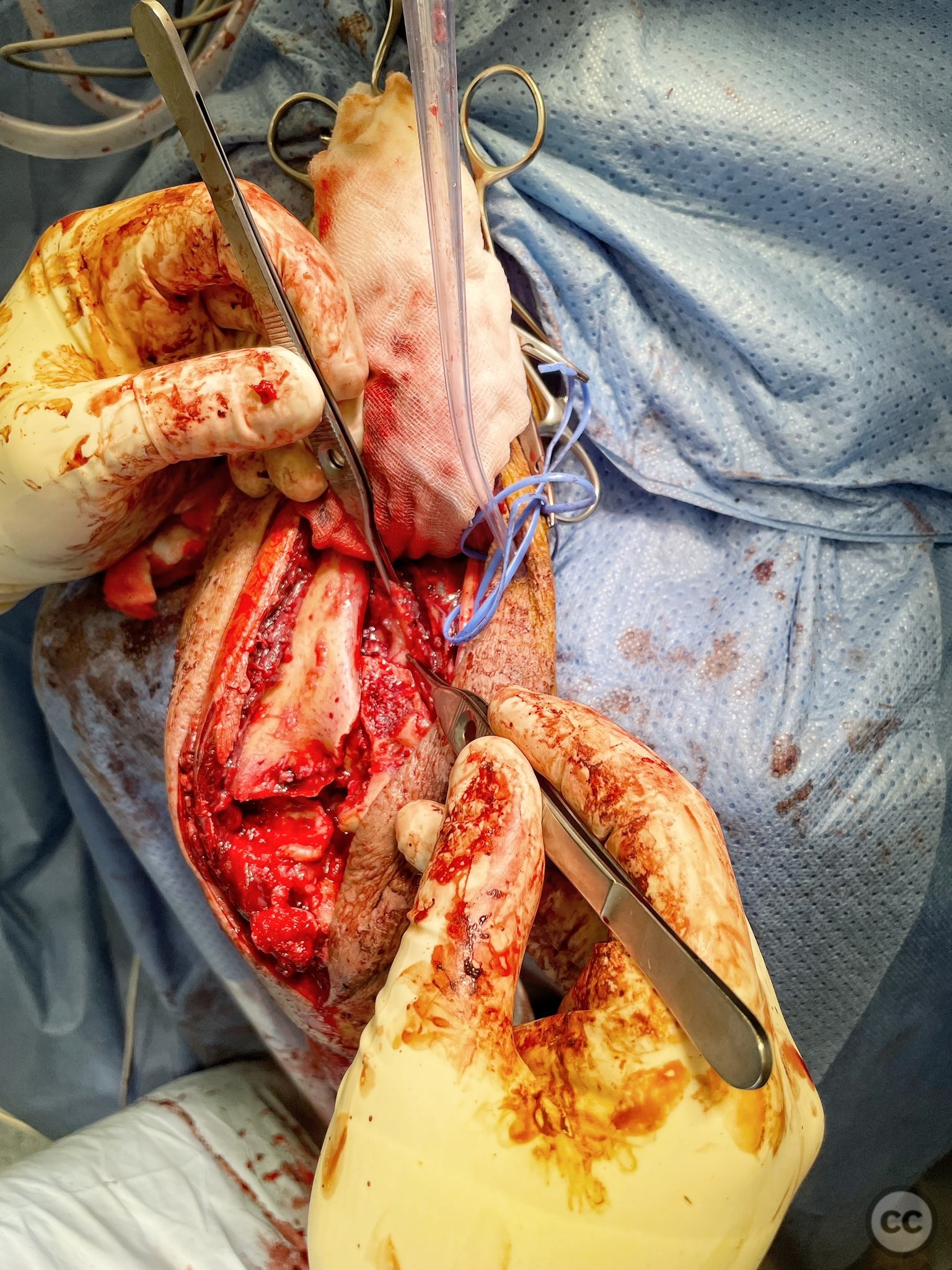
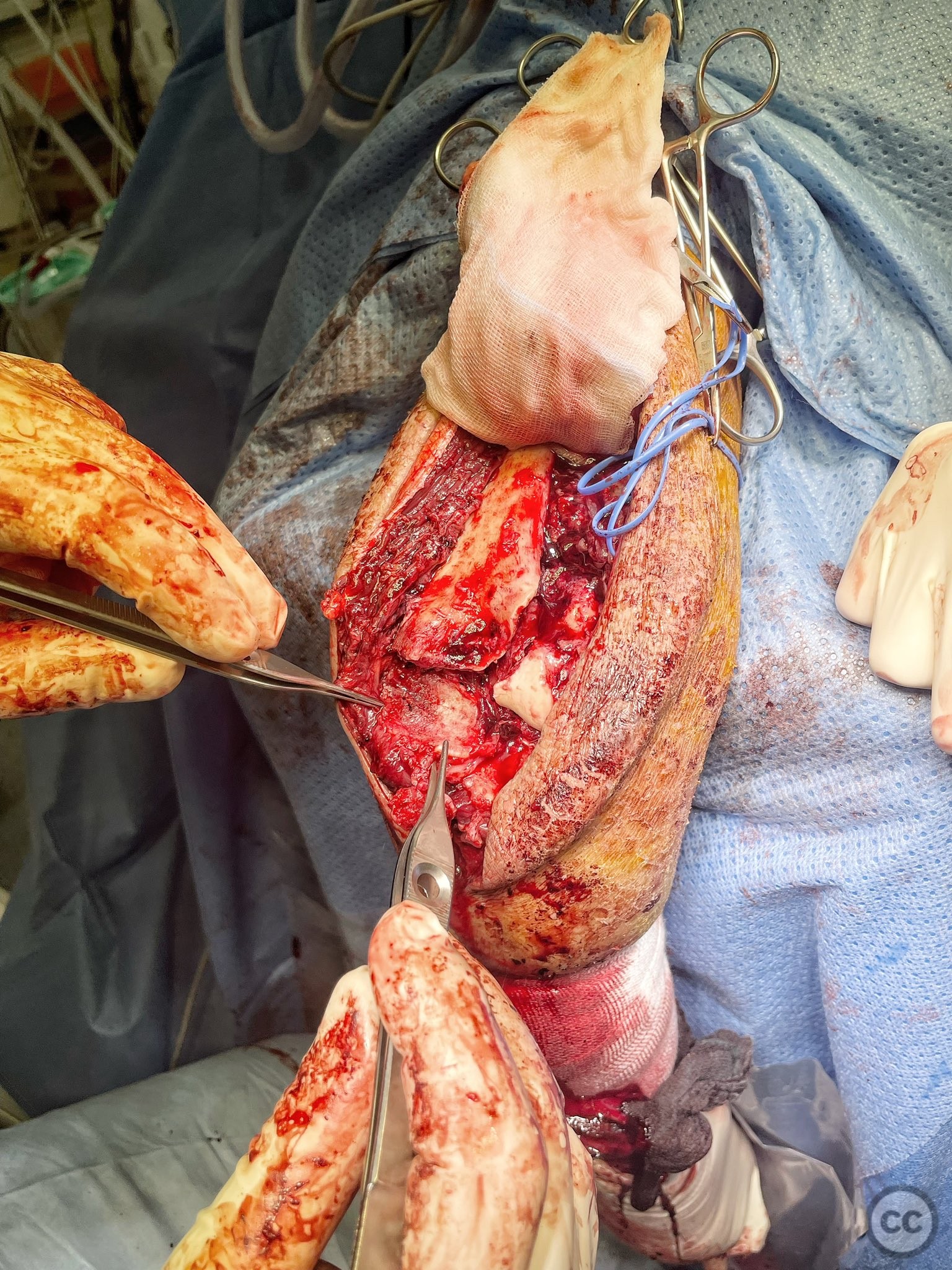
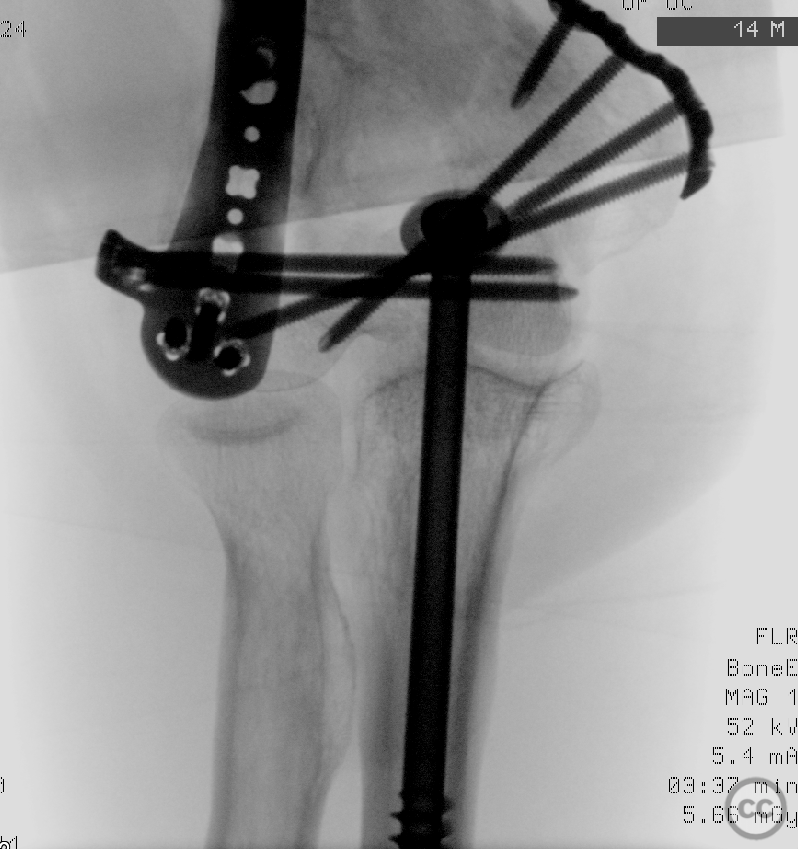
Operative remarks:This is a good case demonstrating my osteotomy technique. I close my osteotomies with a single 7.3 mm cannulated screw. So before cutting the chevron I insert a longitudinal wire for a 7.3mm cannulated screw and over-drill into the proximal aspect of the the ulna diaphysis. Then under direct visual and fluoroscopic control I bring a k wire perpendicular to the dorsal ulnar surface into the bare area and used this k-wire as a saw guide for a Chevron osteotomy. Reflection of the electron and tricep bulk allowed excellent access for articular debridement and reconstruction. 90-degree plating was used to capture both capitellar and trochlear fragments as well as buttress the ulnar column. No free lag screws were used. Closure of the osteotomy with the planned 7.3 mm cannulated screw was unremarkable. Impressive is the compression at the osteotomy site. I split the triceps fibres longitudinally to allow burying of proximal hardware as much as possible
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 506 times
11 Nov 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). C3 distal humerus with olecranon osteotomy. Journal of Orthopaedic Surgery and Traumatology. Case Report 20968954 Published Online Nov 11 2022.