


















Operative Management of Chauffeur's Fracture with Intraarticular Involvement in a Young Adult
Score and Comment on this Case
Clinical Details
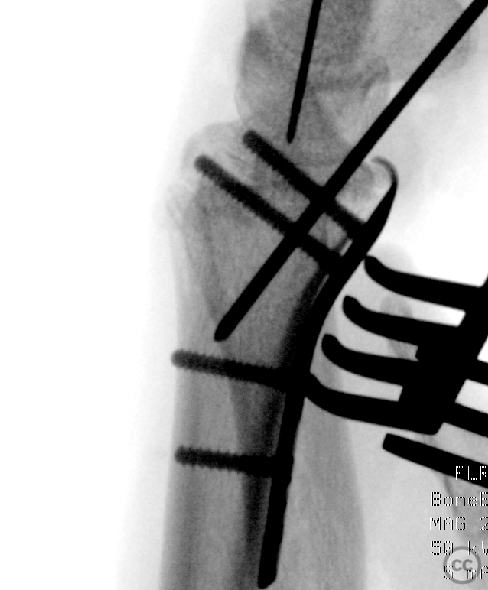
Clinical and radiological findings: A 21-year-old female experienced a low-energy fall resulting in wrist hyperextension and a subsequent left wrist injury. Initial examination and X-ray imaging confirmed a dorsally angulated Chauffeur's fracture, also known as a Hutchinson fracture, along the line of the physeal scar with an intraarticular split and step-off in the lunate facet. CT imaging provided detailed visualization of the fracture's complexity, including a thin lunate rim extension on the volar side.
Preoperative Plan
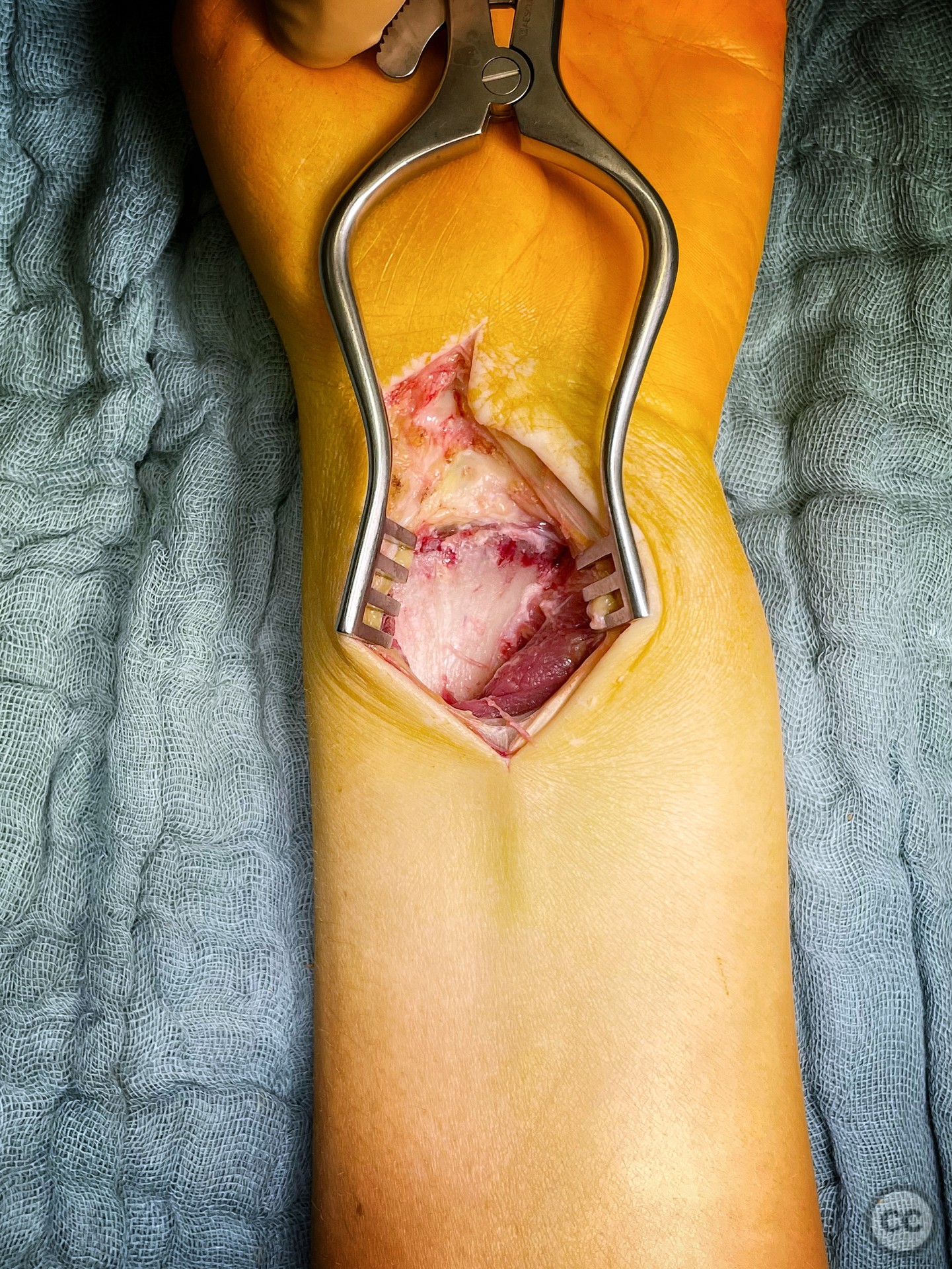
Planning remarks: The preoperative plan focused on restoring the volar tilt of the scaphoid facet and congruency of the lunate facet while reducing any intraarticular step-off. The surgical approach chosen was an extended flexor carpi radialis (E-FCR) modification of Henry's approach, which allows for excellent distal and ulnar visualization.
Surgical Discussion
Patient positioning: The patient was positioned supine with the arm on a hand table.
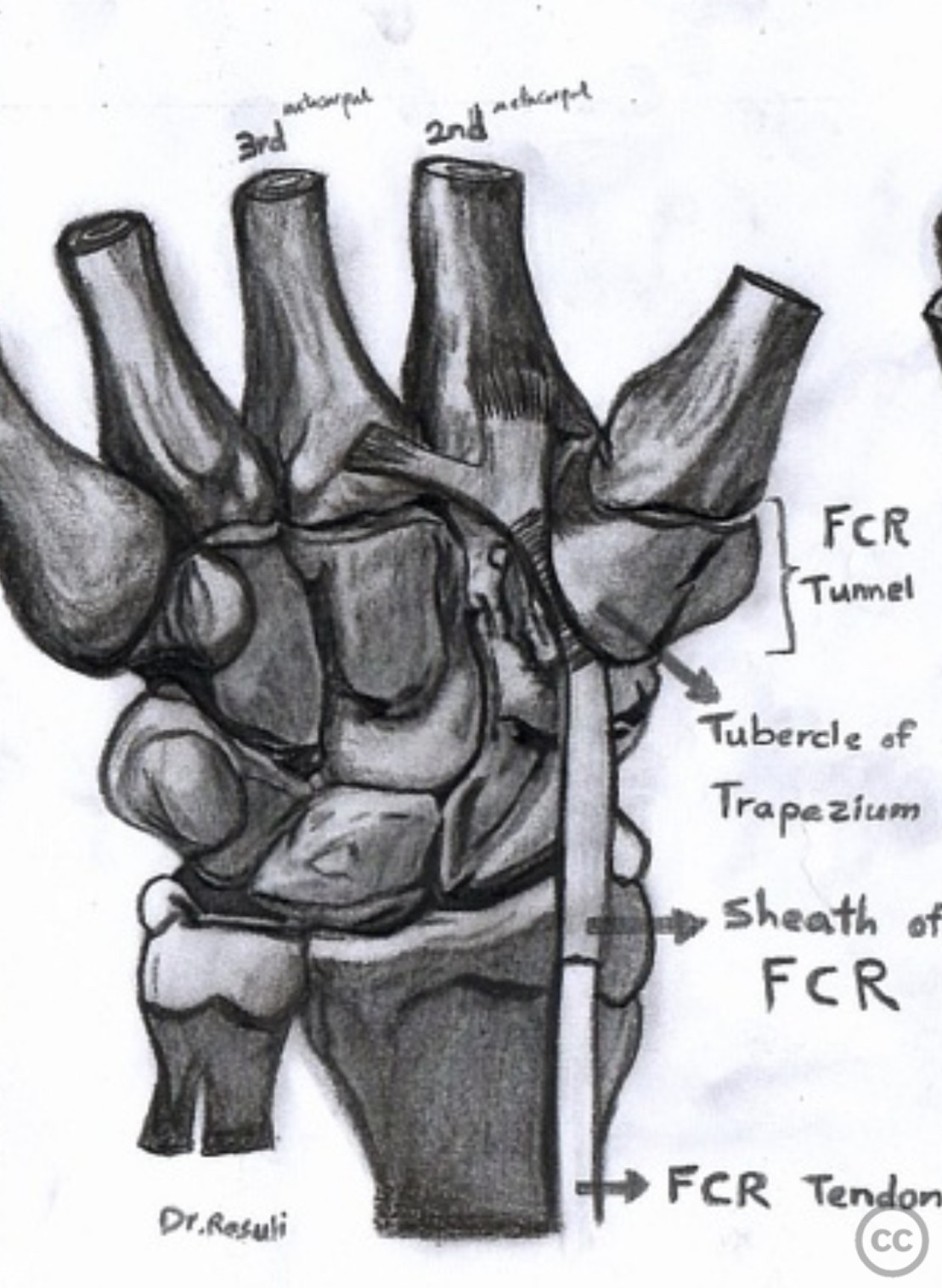
Anatomical surgical approach: The E-FCR approach was utilized, beginning with an incision along the flexor carpi radialis tendon. Dissection proceeded to elevate the pronator quadratus muscle and expose the fracture site while maintaining the integrity of the volar capsular attachments on the distal fragment. Mobilization of the articular fragment was achieved using an osteotome, followed by provisional fixation with K-wires from volar, radial, and dorsal aspects to stabilize multiple axes.
Operative remarks:During surgery, careful mobilization of the articular fragment was achieved leveraging on the lade of a thin osteotome. Provisional fixation with K-wires provided stability across multiple axes. An Aptus volar rim plate, designed for the contralateral side, was selected for its ability to engage a solid edge of the central volar rim effectively. This was followed by further reduction and compression over the plate, with screws directed towards the radial styloid to provide angular stability in good bone quality. An additional 3.0mm headless compression screw was placed over the radial styloid to stabilize the main fracture axis.
Postoperative protocol: Postoperatively, no splint was applied to encourage early mobilization. The patient was instructed on non-weight bearing functional range of motion exercises for 6 weeks.
Follow up: Not specified
Orthopaedic implants used: Aptus volar rim plate, K-wires, 3.0mm headless compression screw.
PubMed® Literature Review
Generated by The Literature - Realtime PubMed® AnalysisThe palmar cutaneous branch of the median nerve (PCBMN) exhibits significant anatomical variability that has critical implications for surgical interventions in the wrist and hand region. Anatomical variations can influence surgical approaches, risk assessment for iatrogenic injury, and diagnostic evaluations [1-12].
The PCBMN typically originates from the radial side of the median nerve but may exhibit several variations concerning its origin point relative to fixed anatomical landmarks such as the distal wrist crease or palmaris longus tendon [4], [6]. Its branching pattern is highly variable; it may bifurcate into radial and ulnar branches at different distances proximal to the distal wrist crease [6], [10]. This variability necessitates a careful dissection during surgeries like carpal tunnel release or volar approach procedures for fractures to avoid inadvertent damage leading to sensory deficits or painful neuromas postoperatively.
Several studies have documented anomalous courses of PCBMN relative to other structures such as flexor carpi radialis (FCR), where it might run superficially, within its sheath, or cross over it in unusual patterns [3], [7], [9]. Such anomalies significantly increase the risk of iatrogenic injury during common orthopedic procedures like open reduction internal fixation (ORIF) for distal radius fractures when using FCR approaches. Glickel et al. reported an incidence rate of approximately 18.8% concerning anomalous branching patterns around FCR sheath based on their prospective study findings, suggesting these variations are more common than previously thought [7].
Furthermore, ultrasonographic evaluation has emerged as a valuable tool in preoperative planning by identifying normal and variant anatomy thereby potentially reducing risks associated with surgical intervention on or near the median nerve including its palmar cutaneous branch. Nulle et al.'s work underscores this utility by highlighting how ultrasound can reveal variants that may not be well-documented otherwise due to their rarity or subclinical presentation until surgically encountered [5].
Given these complexities surrounding PCBMN's course and relationships with adjacent structures coupled with potential functional consequences following iatrogenic injuries - adopting strategies aimed at minimizing risks becomes paramount. Recommendations include utilizing detailed preoperative imaging techniques like high-resolution ultrasound when feasible alongside employing refined surgical techniques that prioritize nerve preservation through enhanced visibility via magnification aids during dissections within high-risk zones identified through anatomic studies discussed herein.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1059 times
10 May 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Operative Management of Chauffeur's Fracture with Intraarticular Involvement in a Young Adult. Journal of Orthopaedic Surgery and Traumatology. Case Report 23233743 Published Online May 10 2024.