





O'Driscoll type 3 coronoid fracture dislocation
Score and Comment on this Case
Clinical Details
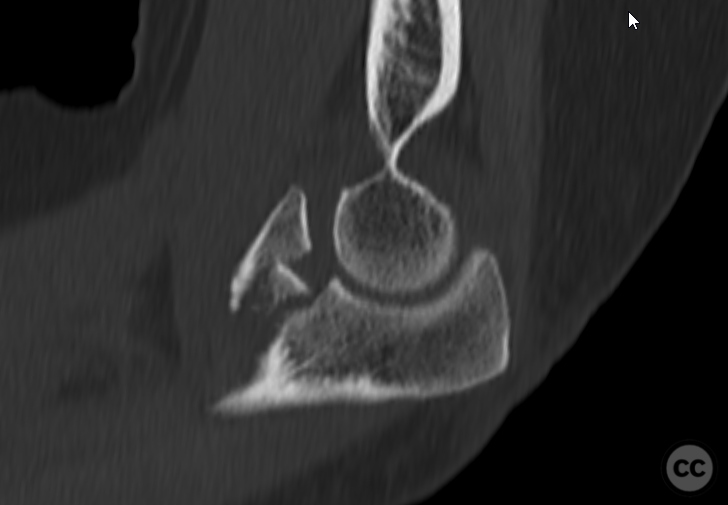
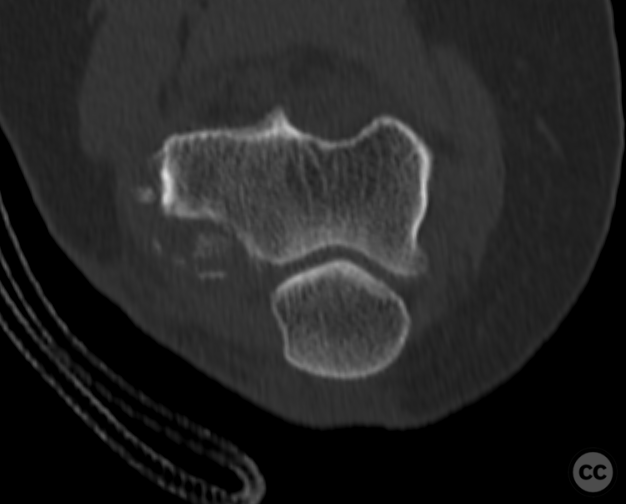
Clinical and radiological findings: The following is a isolated fracture dislocation of the right elbow following fall from standing height in a 60 year old overweight female. The patient presented initially with a posterolateral dislocation which was reduced in the emergency department and subsequently imaged with CT. In CT we can appreciate and O'Driscoll type 3 coronal fracture which extends medially to the level of the sublime tubercle without tubercle involvement. Laterally a bony avulsion of the humeral origin of the lateral collateral ligament is evident.
Preoperative Plan
Planning remarks:
Surgical Discussion
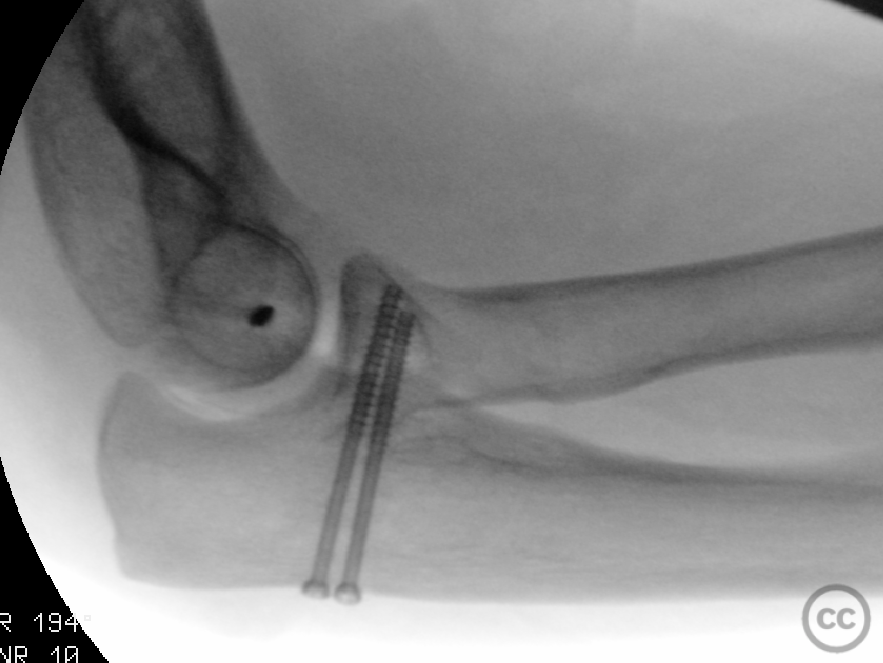
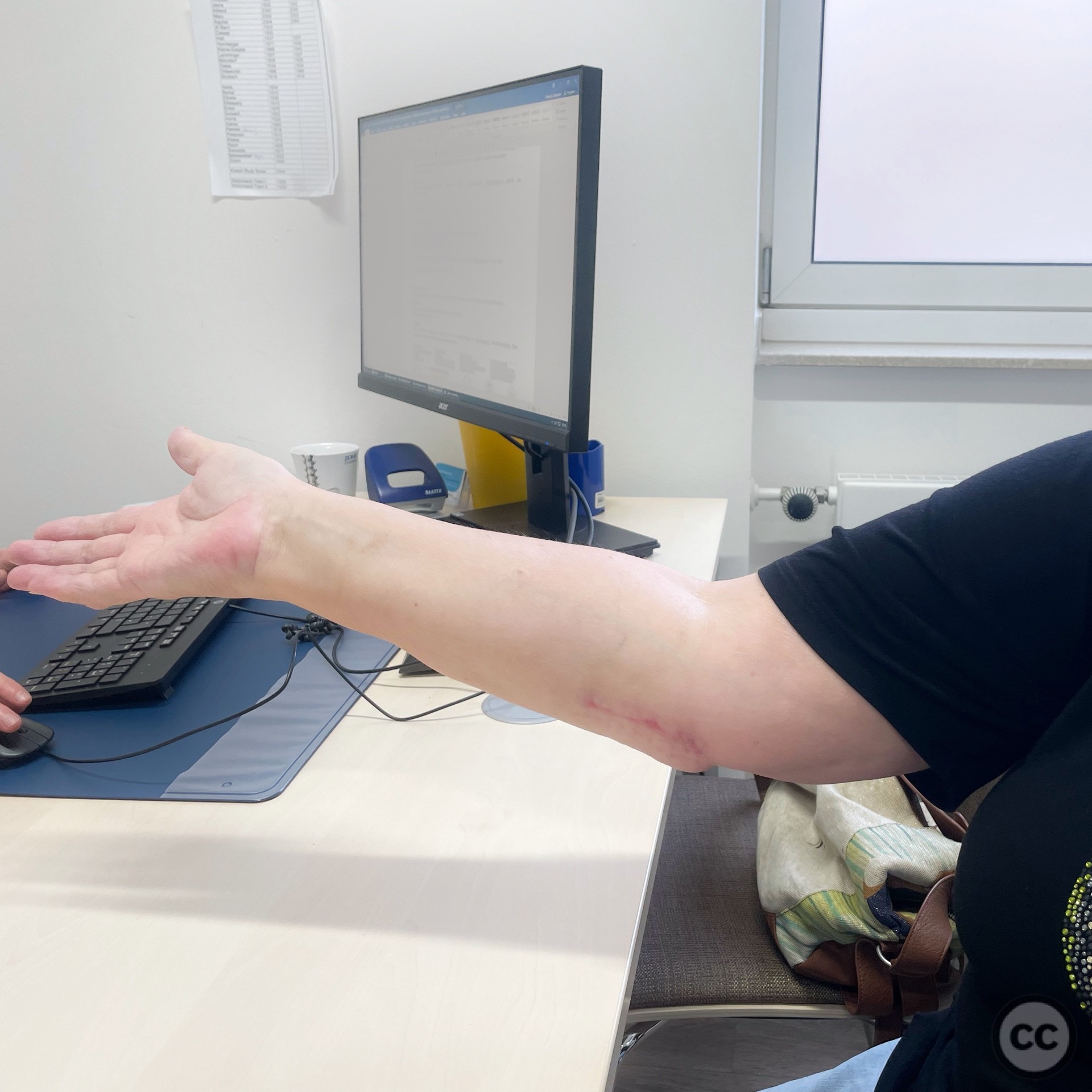
Operative remarks:The operation was performed supine on a radio translucent table. The arm was draped freely and positioned to the side of the patient on a small table. Surgical approach commenced laterally with limited Kocher approach between and anconeus and extensor carpi ulnaris demonstrating a focal bony avulsion of the lcl complex. No articular radial head nor coronoid chondral injury was identified. The lateral collateral complex was re fixed with a single bony suture anchor. Moving medially an approach between the heads of flexor carpi ulnaris into the bed of the ulnar nerve was utilised to gain access above the medial collateral ligament to the coronoid. The coronoid was slightly comminuted but could be reduced well under direct vision. As it was a single large bony fragment the coronoid was able to be fixed with two from posterior to anterior 3.0 mm cannulated screws. It would appear on fluoroscopy that some reduction was lost upon engaging the screws. The visible coronoid and it's reduction (as could be appreciated from the medial approach) however appeared anatomical. one can only assume there is some lateral loss of reduction which could not be appreciated from the media window. The anterior-posterior and oblique views could not identify the degree of malreduction and the joint surface as visualized laterally appear congruent and step free. Additionally the intra-operative dynamic stability of the joint was not compromised. A passive congruent range of motion from 0 20-120 degrees could be demonstrated on the table. At the post-operative review at 6 weeks the patient had a functional arc of over 100 degrees and was very pleased with the clinical result.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1105 times
08 Nov 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). O'Driscoll type 3 coronoid fracture dislocation. Journal of Orthopaedic Surgery and Traumatology. Case Report 24520919 Published Online Nov 08 2022.