







AO/OTA 43-C3 Pilon Fracture through a posterolateral approach
Score and Comment on this Case
Clinical Details
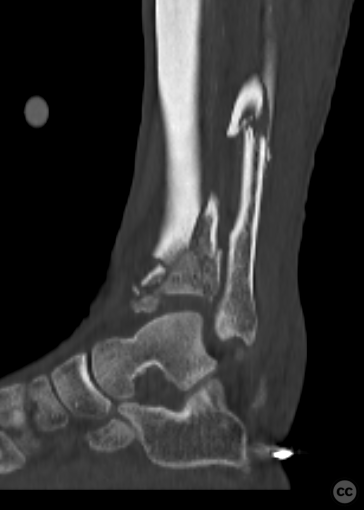
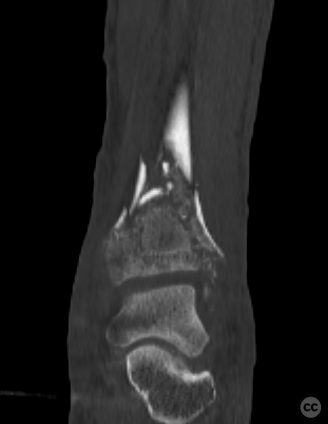
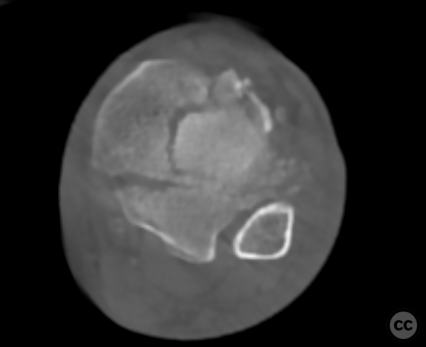
Clinical and radiological findings: A 65-year-old male polytrauma patient following a fall from scaffolding >5 meters. The patient sustained multiple axial skeletal injuries, with a pilon fracture identified during initial polytrauma CT screening. An external fixator was placed during the initial stabilization of other injuries.
Preoperative Plan
Planning remarks: The planned surgical approach involved a two-phase procedure. The first phase utilized a posterolateral approach to the distal tibia and fibula for fracture reduction and fixation. The second phase involved supine repositioning anda medial approach to address the medial malleolus together with syndesmotic stabilization.
Surgical Discussion
Patient positioning: Initially prone with the left limb secured in an external fixator device, supported by a carbon fiber roll under the external fixator frame at the level of the left ankle. The second phase involved repositioning to supine for medial approach and removal o
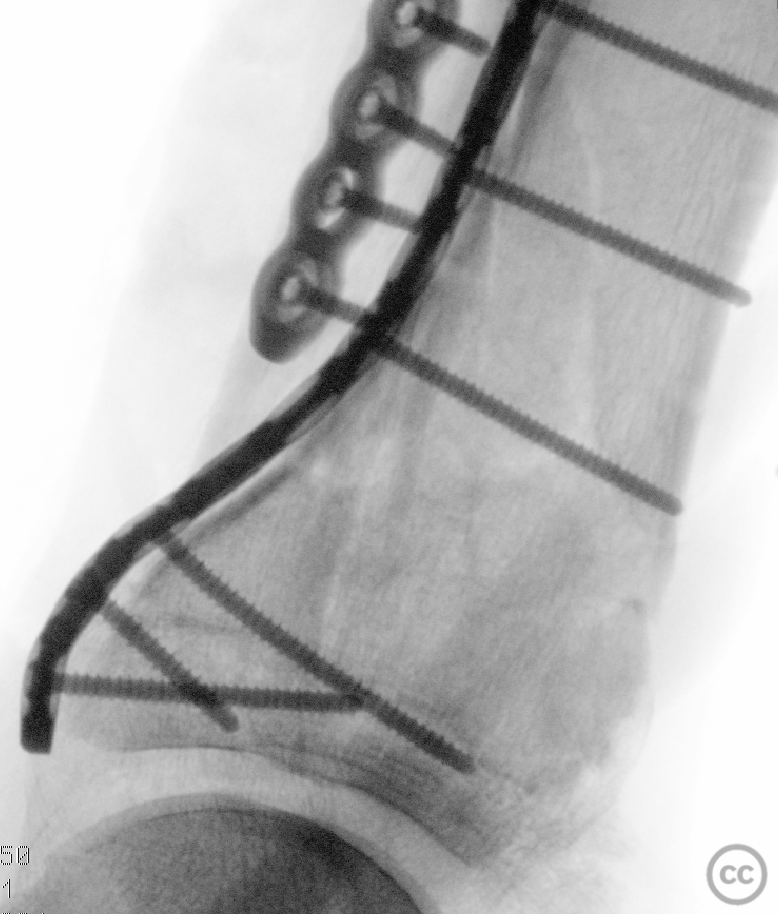
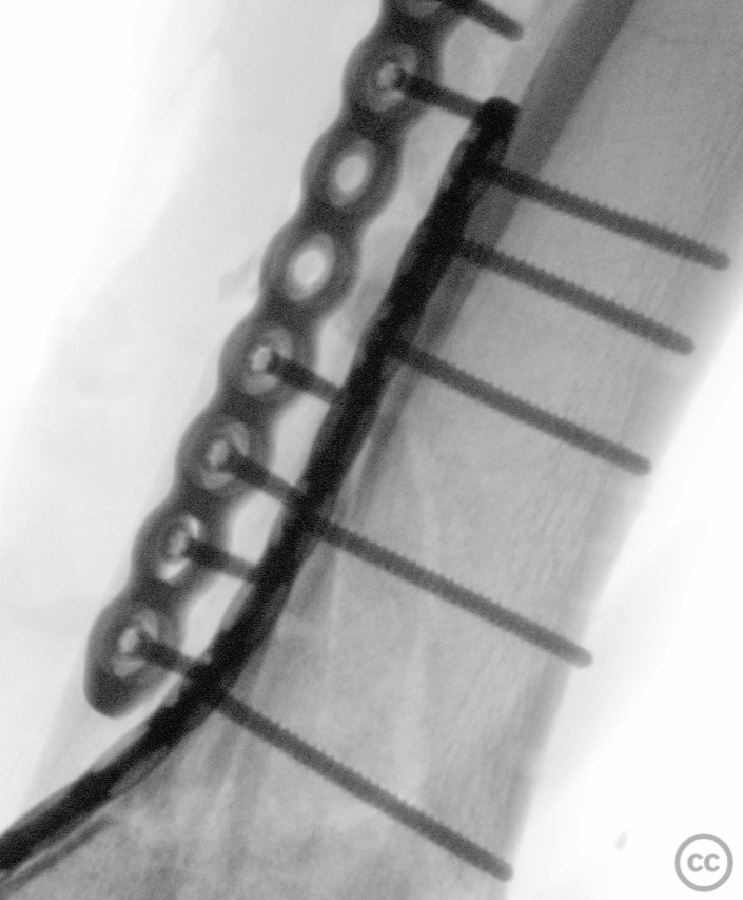
Anatomical surgical approach: A longitudinal incision was made over the posterolateral aspect of the distal tibia. Subcutaneous dissection exposed and retracted the sural nerve medially. The anatomical plane between the peroneus muscles and flexor hallucis longus was identified, allowing blunt dissection towards the posterolateral cortical margin of the distal tibia. Partial sharp dissection of flexor hallucis longus from its attachment on the posterior aspect of fibula provided exposure for accessing two-thirds of the tibial surface down to joint level. The fibula was exposed by circumnavigating lateral aspects of peroneal muscles, raising a full-thickness flap, and reducing and stabilizing fracture sites with a 2.7 mm mini fragment locking plate. The second phase involved a direct medial approach to the medial malleolus, revealing fracture complexities and securing with a medial distal 3.5 mm locking plate.
Operative remarks:Despite moderate callus formation around multiple bony fragments limiting mobilization, debridement and sequential mobilization were feasible. Achieving complete anatomical reduction of the tibial plafond while maintaining positioning within the external fixation frame proved unattainable through manipulation alone. Provisional stabilization using K-wires allowed for de-rotation and restoration to physiological length before affixing a pre-contoured 12-hole 2.7 mm mini fragment plate along the posterolateral margin. Given extensive comminution rendering anterolateral rim unsuitable for plating reconstruction, limited exposure facilitated fragment-specific fixation enhancing cortical contour restoration at anterolateral corner albeit without directly addressing main comminution at joint level due to involvement with anterior syndesmotic fibers origin necessitating percutaneous insertion of a 3.5 mm syndesmosis screw stabilizing fibula-tibia interface promoting secondary bone healing without direct fixation need.
Postoperative protocol: Not specified
Follow up: Not specified
Orthopaedic implants used: - 2.7 mm mini fragment locking plate - 3.5 mm medial distal locking plate - 3.5 mm syndesmosis screw - K-wires
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 259 times
17 Jul 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). AO/OTA 43-C3 Pilon Fracture through a posterolateral approach. Journal of Orthopaedic Surgery and Traumatology. Case Report 24652049 Published Online Jul 17 2024.