

Monteggia like fracture dislocation with coronoid fracture
Score and Comment on this Case
Clinical Details
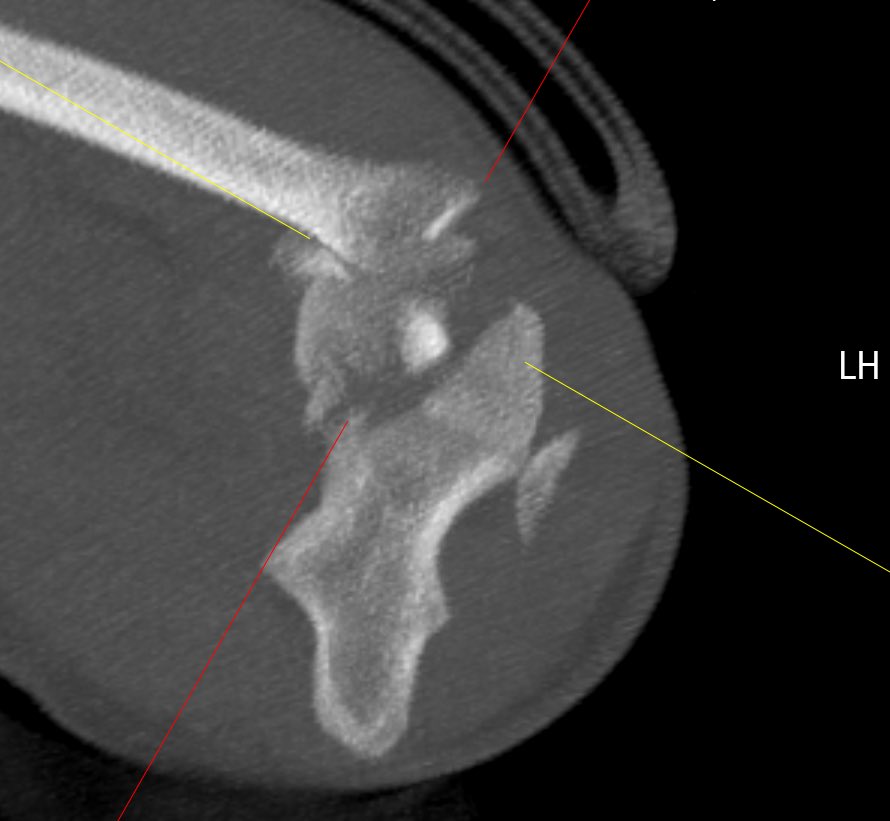
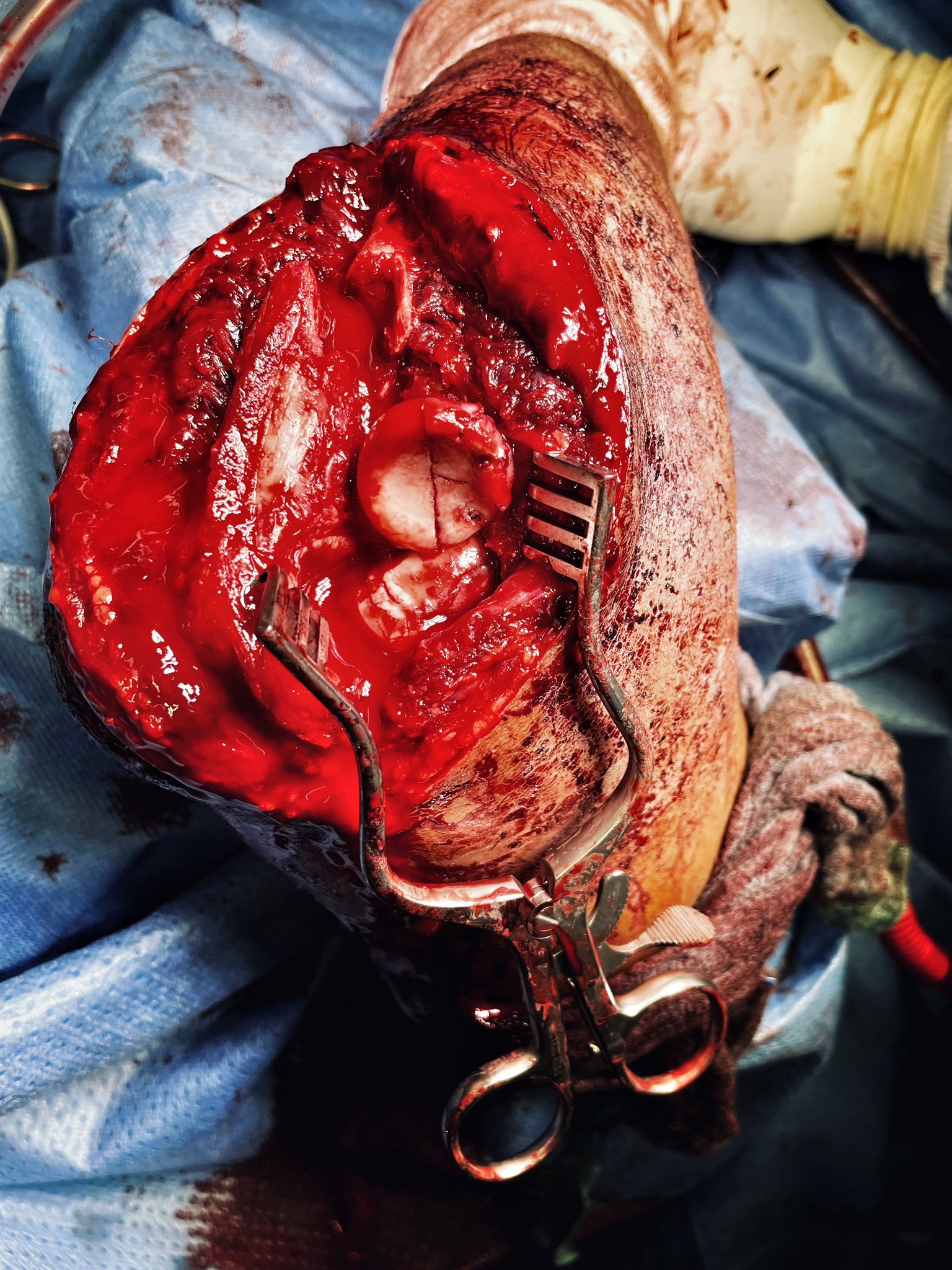
Clinical and radiological findings: This Montagia like lesion (a true Montagia fracture dislocation is defined by a disruption of the proximal radioulnar joint) involves comminuted fractures of the radial head and capitellum with entrapment of a fragment of the radial head between capitellum and distal humerus. The long axis of the radius remains in a dorsally dislocated position together with a subluxed position of the proximal olecranon/humeroulnar joint. The dorsal orientation of this injury loans itself to a dorsally oriented surgical approach. Here the dorsal Boyd's approach be can used to advantage.
Preoperative Plan
Planning remarks:
Surgical Discussion
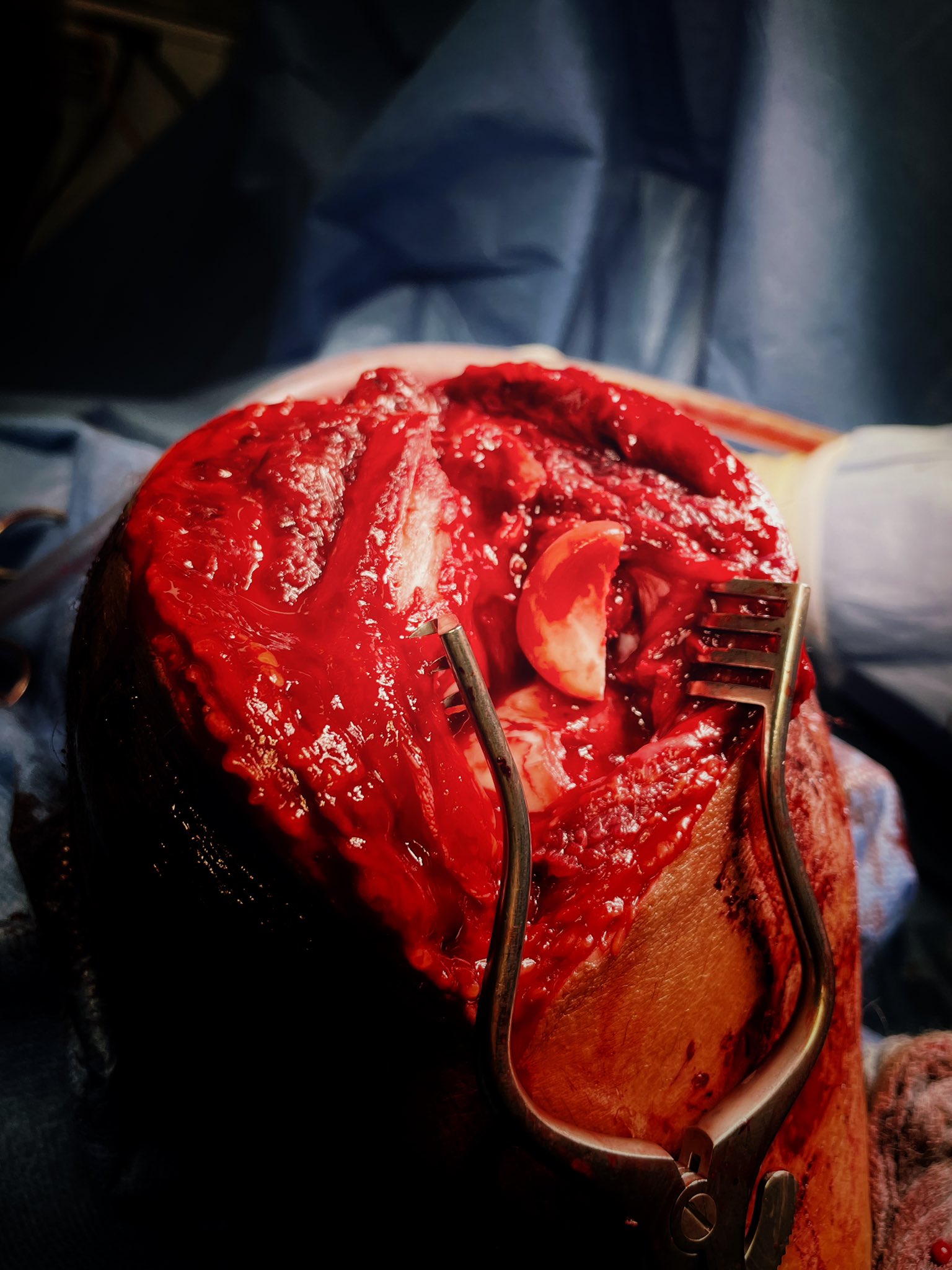
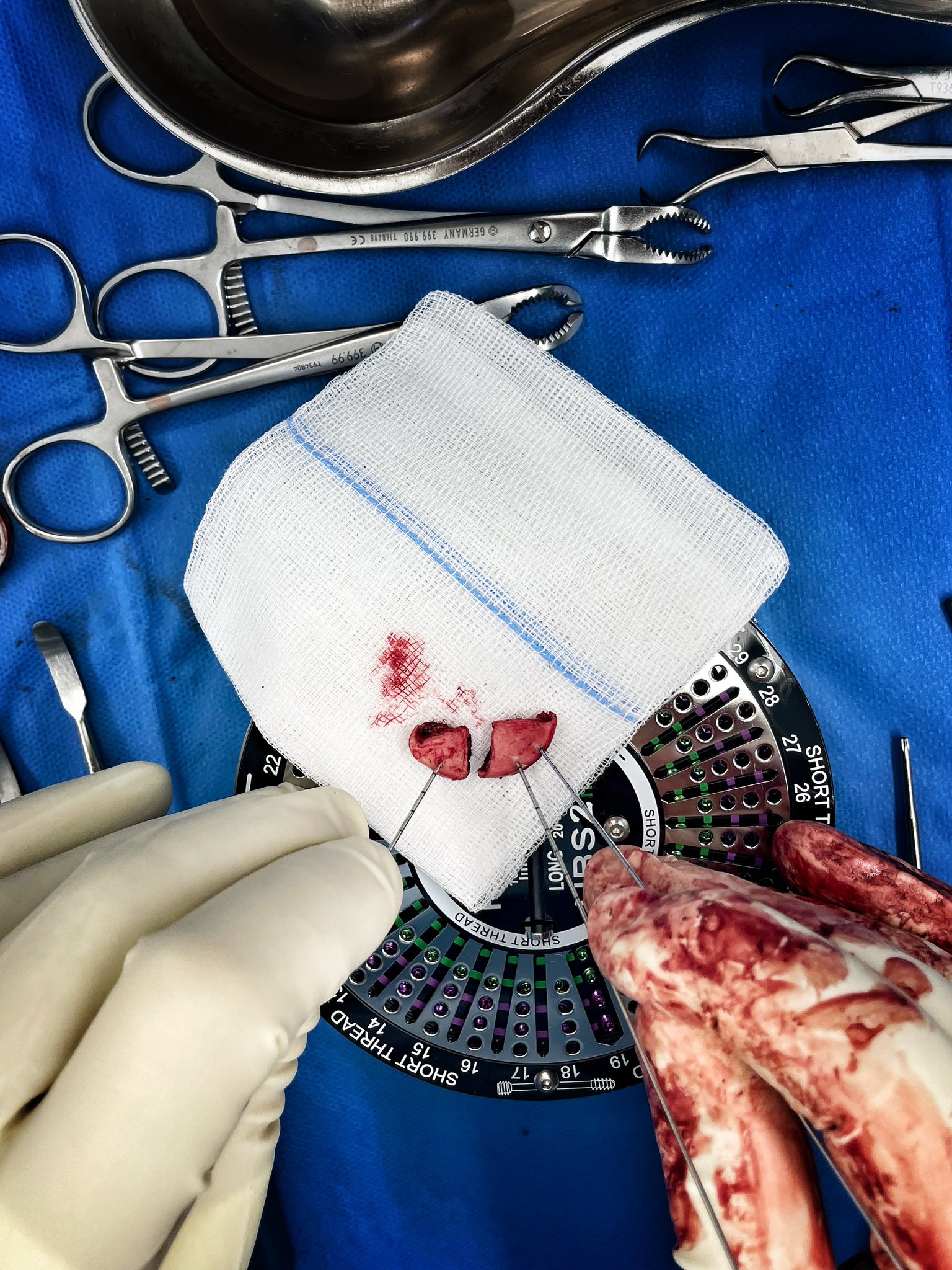
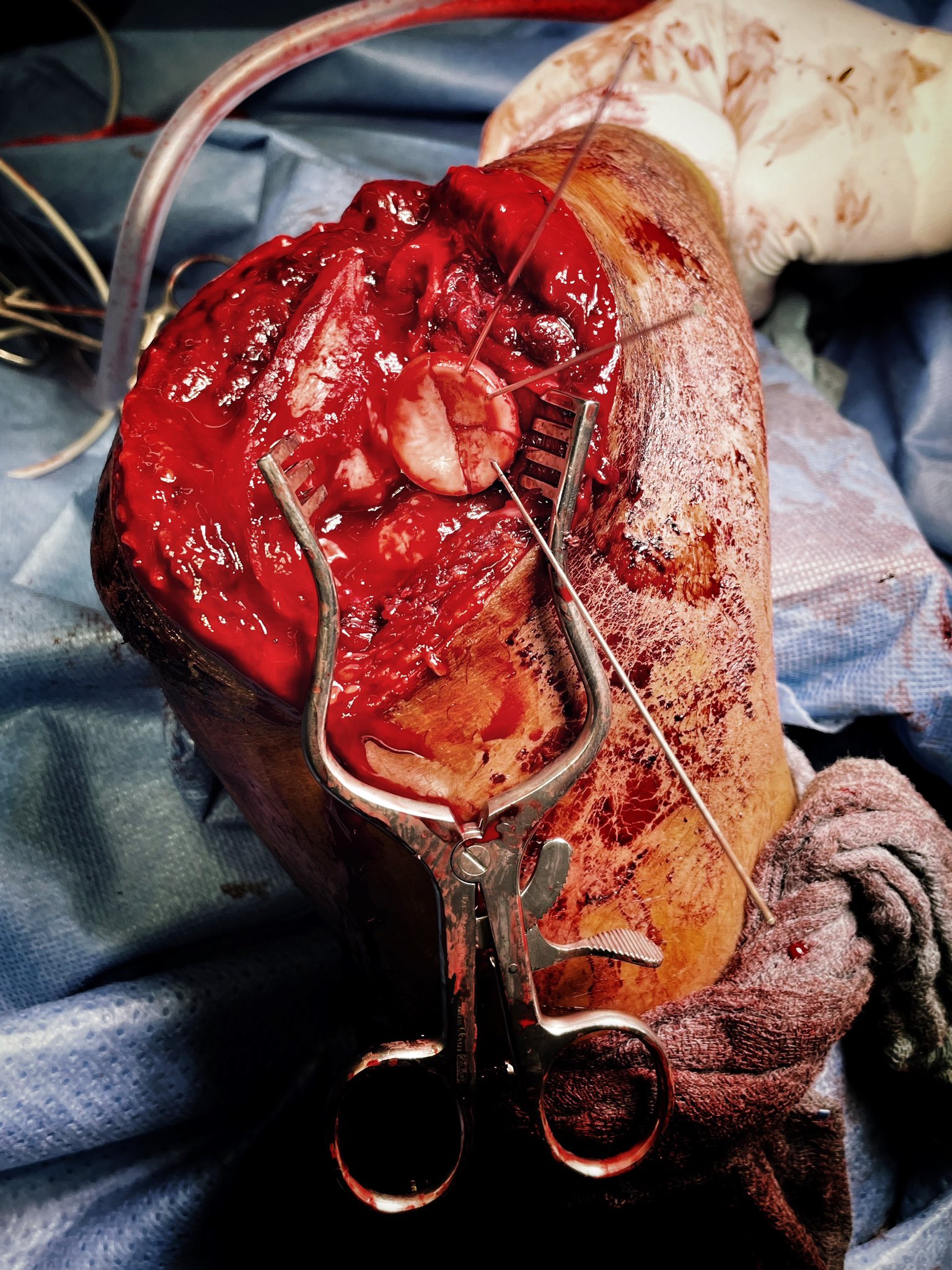
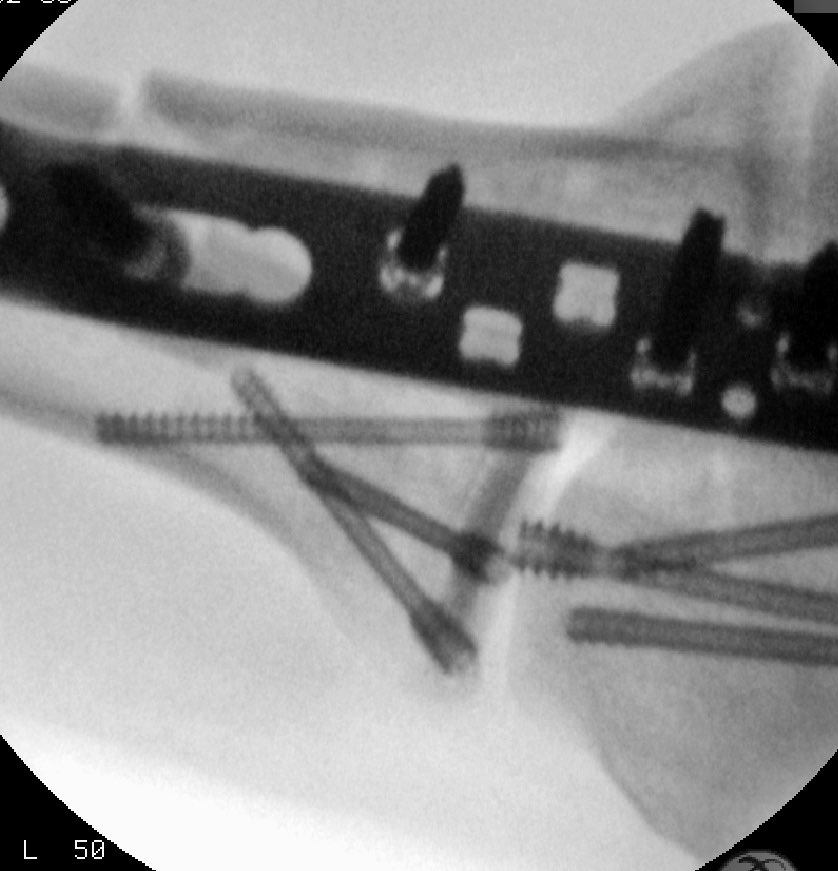
Operative remarks:The patient was positioned supine with the injured arm resting on a small support across the patient’s chest. A tourniquet was placed around the proximal humerus. A longitudinal incision centred along the proximal ulna curving radially over the olecranon into the distal humerus was utilized. Following subcutaneous dissection, anconeus was divided from the radial border of the ulna down onto the lateral ulnar collateral ligament and ligamentum annularis. Subperiosteal elevation medially in a limited Taylor-Scham approach was be used to help visualise and reduce the ulnar fracture. To open Boyds interval we sharp dissect the ligamentum annularis and the ulnar insertion of the lateral ulnar collateral ligament from the supinator ridge. In combination with the ulnar fracture (providing dorsal instability of the ulna column) division of the lateral collateral ligament and annular ligament allows a complete dorsal dislocation of the radial shaft and head. The clinical photos demonstrate the dislocated radial head as seen from the perspective of the operating surgeon. The head fragments were disimpacted from under the capitellum or retrieved out of the joint, reassembled on the back table, and then reassembled to the residual intact head and neck using a tripod technique of headless bone screw fixation. A loss of bone substance immediately under the head fragments excluded the use of plate fixation. Once disimpacted the capitellar fracture could be similarly reduced under direct vision. Following temporary fixation utilizing k-wires we performed definitive screw fixation using poster-anterior and anterior-posterior headless bone screws. With anatomical reduction of head and capitellum, the radiocapitallar joint could be congruently reduced. The ulnar fracture was then reduced and plated with a proximal olecranon locking plate. Refixation of the lateral ulnar collateral ligament and ligamentum annularis was done through transosseous drill holes traversing the ulna from medial to lateral and exiting the supinator ridge. Here we used 2 strand ultrabraid krackow suture pulled transosseously and tied at the ulna aspect of the olecranon. This provided an intra-operative stable osteosynthesis allowing full passive range of motion in flexion extension and supination and pronation without residual instability.
In my opinion this is the perfect indication for a Boyd approach (or Writington) to the elbow joint. Boyd's interval allows concomitant osteosynthestic management of the distal humerus and radial fractures as well as parallel fixation of the ulnar fracture. The transosseous refixation of the ligamentum annularis and lateral ulnar collateral ligament is a mechanically sound construct and superior to intra-substance repair as would be necessary through a dedicated Kocher or Kaplan interval to the radial head. The novel tripod fixation technique of radial head fragments is described in the literature. Biomechanically a tripod construct has been shown to tolerate excellent axial loading of the joint without the bulky peripheral hardware associated with plate osteosynthesis.
Orthopaedic implants used: Synthes 3.5/2.7mm Olecranon locking plate. HBS Midi Headless Bone Screws
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1047 times
03 May 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Monteggia like fracture dislocation with coronoid fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 24849715 Published Online May 03 2022.