

Retrograde IM screw fixation of an isolated Weber A fracture
Score and Comment on this Case
Clinical Details
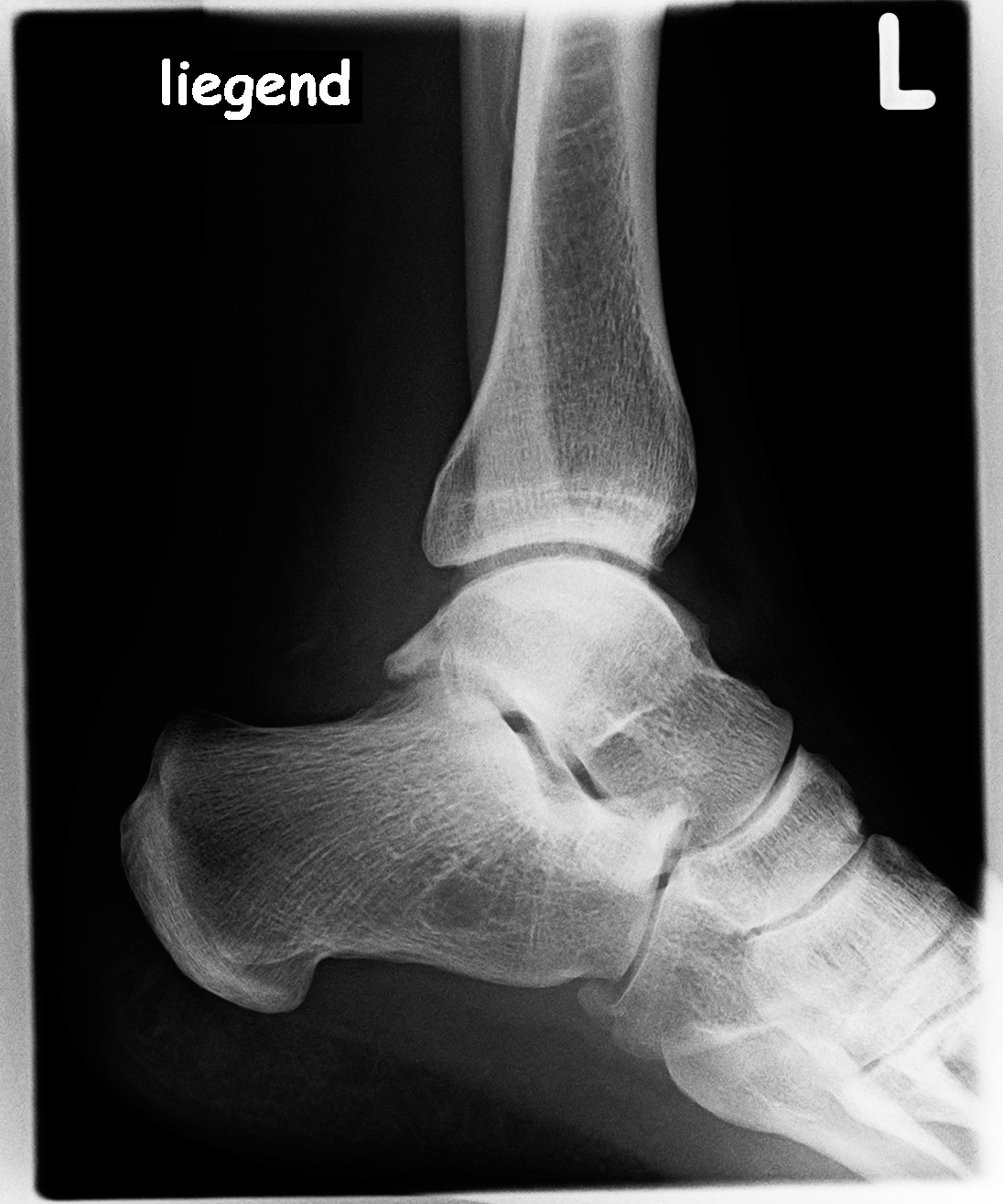
Clinical and radiological findings: This is a bit of an uncommon problem - a 38 year old male following a simple supination injury and subsequent large displaced Weber A avulsion fracture of the distal fibula. As identifiable on the pre operative plain film imaging - this is an atypically large fragment which has significant (>2 mm) of lateral displacement. The operation took place supine with the lower limb internally rotated through a wedge under the left hemi pelvis, the limb prepped and draped as usual. I used a limited direct lateral approach to the distal aspect of the fibula with minimal soft tissue dissection. Reduction and fixational of the fracture over a K wire was unremarkable.
Preoperative Plan
Planning remarks:
Surgical Discussion
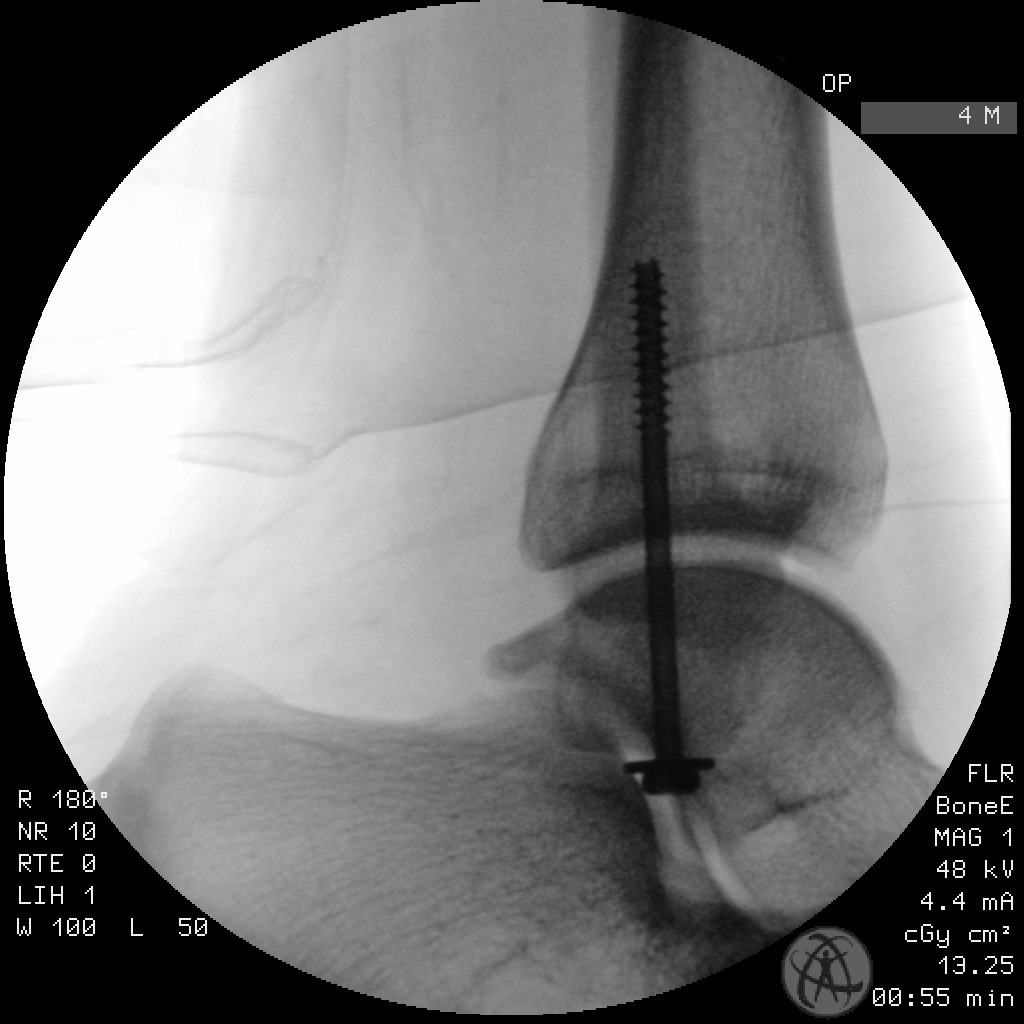
Operative remarks:I had neither seen this patient in the clinic nor had I been made aware of him subsequent to his initial presentation to the emergency department (there's downsides to working in a large trauma centre sometimes I guess). He simply appeared on one of my operative lists one morning and this was the first I'd had the opportunity to think about how I was going to fix it. Of the various operative possibilities that came to mind, I was tending towards a distal fibula locking plate - before it occurred to me that a simple cannulated screw fixation wasn't actually a bad idea. I often use simple cannulated screw fixation for fifth metatarsal avulsion fractures - and this fracture didn’t strike me as particularly different to those that we see commonly in the midfoot. The fracture provided enough interdigitation in itself to be rotationally stable and the compression provided by the screw (with the screw threads biting well into proximal cortical bone) was quite significant. The peroneal tendons were not disturbed by the position of the screw head and washer. So perhaps a bit unusual, but given the anatomic reduction and stable fixation with great compression provided by the screw, I'm quite content with the result. There is very little literature to support this approach. See Reference links.
Orthopaedic implants used: 4.5mm cannulated titanium screw
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1423 times
21 Mar 2021
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2021). Retrograde IM screw fixation of an isolated Weber A fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 24860866 Published Online Mar 21 2021.