











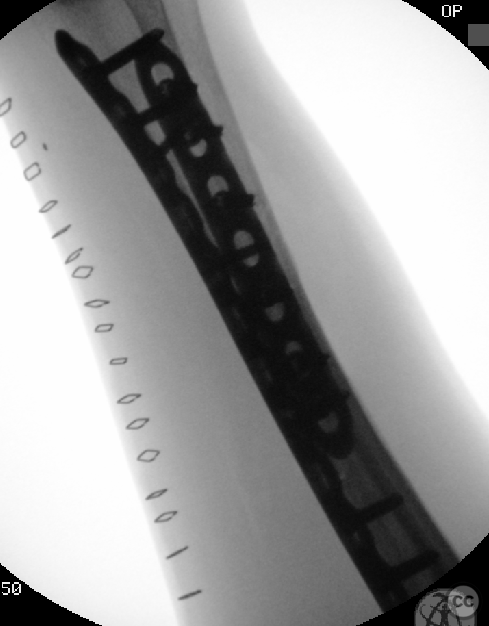


Henry's approach to a segmental radial shaft fracture
Score and Comment on this Case
Clinical Details
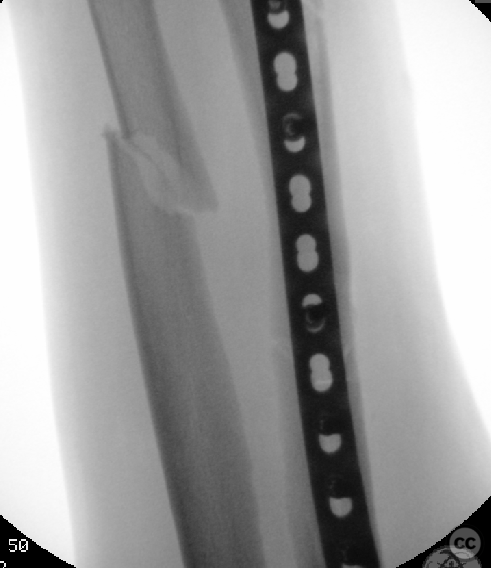
Clinical and radiological findings: This is a 38 year old man who sustained a segmental radial shaft fracture and a concomitant simple ulnar shaft fracture in the context of a motor vehicle rollover accident. There was a soft tissue injury to the dorsal aspect of the proximal forearm and elbow, which was not associated with the bony injury. The bone your injury itself was closed, the hand and distal forearm were neurovascularly intact. The operation was done acutely following initial trauma resuscitation as part of an early definitive care surgical strategy
Preoperative Plan
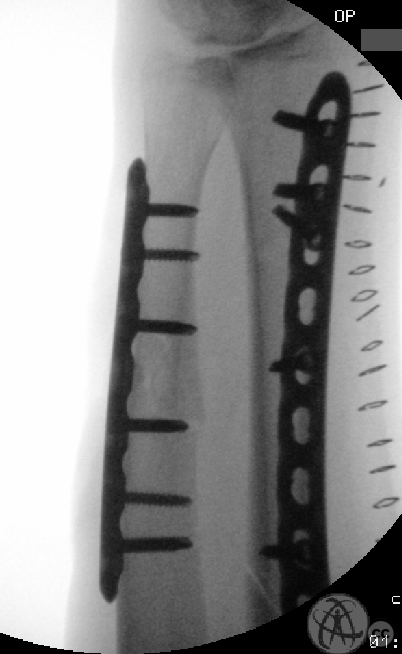
Planning remarks: With a both-bone fracture constellation, one often speaks of managing the simplest fracture first. In this case both fractures were of equal (simple) complexity. The segmental nature of the radial fracture was not considered to increase the surgical complexity, and achieving anatomical reduction should be straight forward. The volar approach to the radial shaft is simpler in terms of patient positioning (when the arm is floppy). Following stable fixation of the radius, the second surgical approach between extensor carpi ularis and flexor carpi ulnaris is simplified
Surgical Discussion
Patient positioning: Supine with the arm on a separate arm table.
Anatomical surgical approach: Modified Henry's approach to the radius. Ulnar approach between FCU and ECU
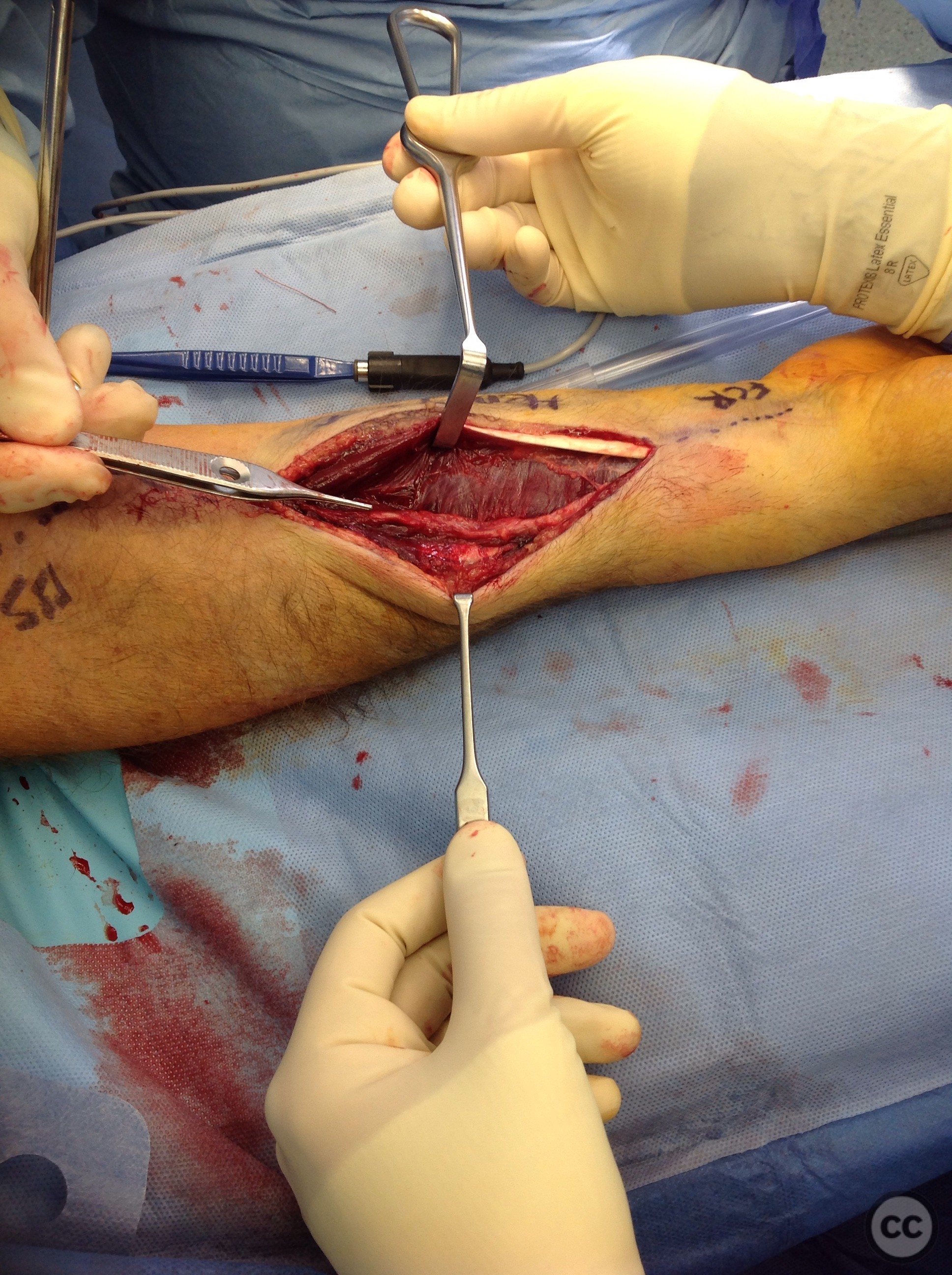
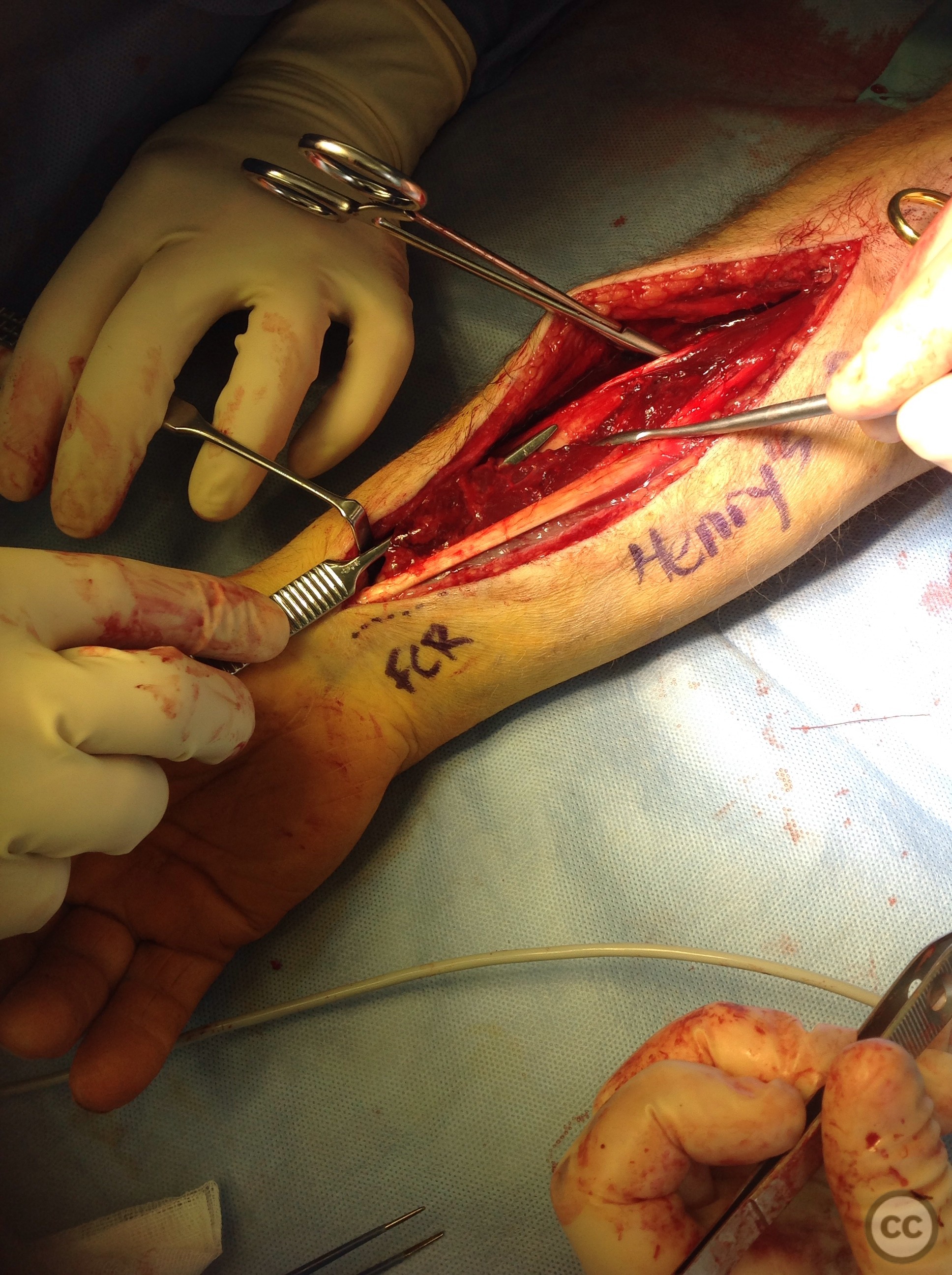
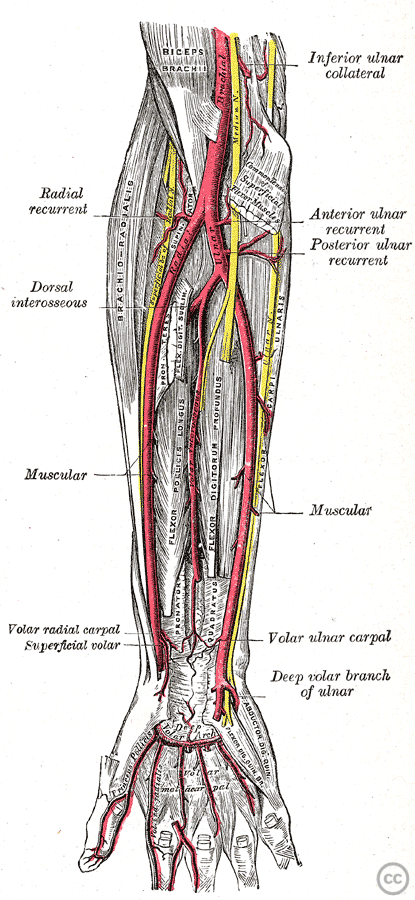
Operative remarks:The textbook Henry's approach identifies a surgical plane between bracioradialis and flexor carpi radialis, with identification and retraction of bracioradialis and the radial nerve radially and flexor carpi radialis and the radial artery taken ulnarly. The modification of Henry's approach involves opening the FCR sheath, retracting FCR ulnarly, and the retraction of the radial artery to the radial side keeping the artery and nerve together. These two structures diverge just distal to the radial tuberosity, with the radial artery coursing ulnarly before continuing into the upper arm as the brachial artery. Preoperative planning will define how how far proximally the surgical approach will be taken, and this may influence whether the artery is mobilised together with either the ulnar or radial structures. In this case, the fracture at midshaft level does not involve significant proximal soft tissue mobilisation such that keeping the neurovascular bundle to the radial side was feasible. Following the establishment of a window between flexor carpi radialis and brachioradialis, identification of the divergent fibers of pronator teres (and flexor digitorum superficialis) and flexor policis longus, followed by retraction of these proximally and disitally respectively, a blunt window of the midshaft of the distal radius it can be demonstrated over a length of around 4 centimetres. Sharp elevation of a limited portion FPL and FDS (to the radial fibers of PT) increases this window to around 8cm without significantly compromising either muscle. I do my best to maintain as much muscular origin as possible and attempt to create several such windows, tunnelling the plate under muscular belly whilst leaving the belly of the muscle itself intact. In the intraoperative photographs, the interval seen is that between FPL distally, and PT proximally, with cut fibers of FPL and FDS visible retracted ulnarly. This transcript was generated by https://otter.ai
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
User Discussion (1)
Guest User
Explains options for handling of the radial artery.