



Pronation Abduction (PAb) Weber C / Herscovici B bimalleolar ankle fracture
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: This is 37yo gentleman who sustained a pronation abduction the right ankle following a twisting fall during a football game. He describes an initial clinical sub/dislocation before spontaneous reduction of the ankle on field. The patient presented acutely to the emergency department end following plain film imaging underwent acute definitive fracture fixation. The pronation abduction type mechanism results in the classical medial avulsion fracture and suprasyndesmotic fracture of the fibula. This constellation implies rupture of the anterior tibiofibular ligament, the interosseous membrane, and a posterior tibiofibular ligament injury. Infact a small posterior bony avulsion is visible on plain film imaging in this case. PTIFL may also be represented by a Mason type 1 or type 2 fracture posterior malleolar fracture (Type IV).
Preoperative Plan
Planning remarks:
Surgical Discussion
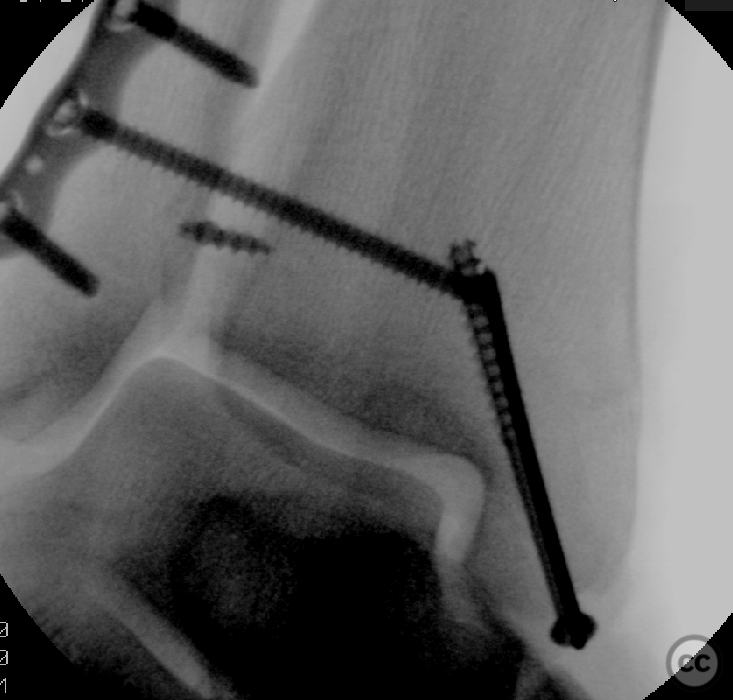
Operative remarks:Patient was positioned supine on a radio translucent table. Initial surgical approach was lateral - there was no indication of static motise shift blocking fibular reduction so we could proceed with primary lateral reduction and fixation. The fibula was relatively simple to reduce and was fixed with a 3.5 mm locking plate. Anterior preparation to the Chaput tubercle and anterolateral tibotalar joint allowed direct reduction of the fibula into the syndesmosis under direct vision. This was temporarily fixed using k-wires, the syndesmosis fibres were avulsed completely from the tibial side and following whip stitch arming of the ligament it was secured back to bone using a suture anchor. To support the reduction a tricortical the screw was introduced. The posterior injury was therefore not addressed directly. Moving to the medial side the Herscovici B fracture was reduced, and due to is relatively small size it was fixed with a 4.0 mm cannulated screw and simple k-wire anti rotation screw.
Orthopaedic implants used: Stryker 3.5mm Ankle System. Arthrex Fasttak Suture Anker.
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1861 times
20 Dec 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Pronation Abduction (PAb) Weber C / Herscovici B bimalleolar ankle fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 26967311 Published Online Dec 20 2022.