









Neglected Intra-Articular Distal Radius Malunion with Ulnar Syndrome
Score and Comment on this Case
Clinical Details
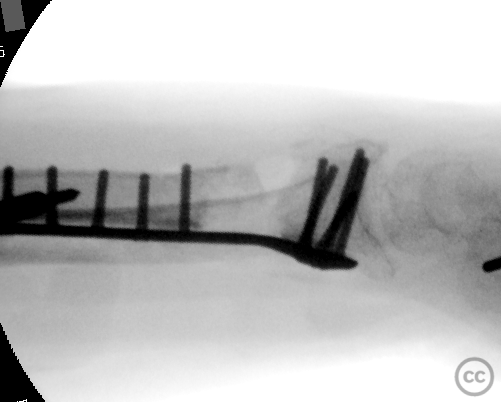
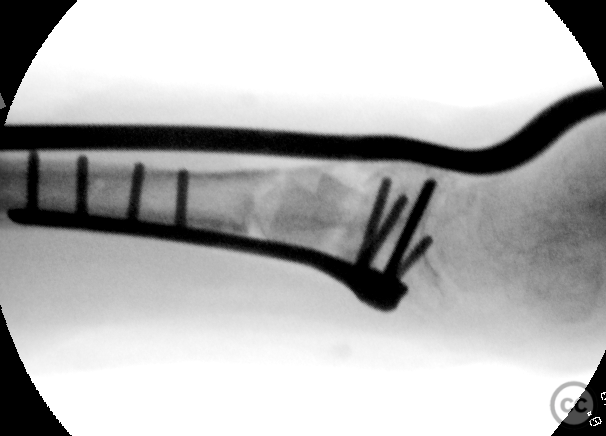
Clinical and radiological findings: A patient of non-English speaking background presented three months post-injury with a neglected displaced intra-articular distal radius fracture on the left side. The fracture had united approximately 30 to 40 millimeters short, resulting in a significant ulnar plus variance. This led to ulnar carpal impaction and significant pain, alongside notable clinical deformity and loss of range of motion. Radiographic imaging demonstrated radial column shortening, fracture imapction and significant subchondral bone loss, alongside generalized disuse osteopenia. CT imaging confirmed a partially non-united but clinically solid malunion.
Preoperative Plan
Planning remarks: The preoperative plan involved a Henry's approach to the distal radius for osteotomy and debridement of the old fracture plane. Distraction was planned using a 2.5 millimeter threaded pin distraction device inserted in the radial diaphysis and second metacarpal shaft. Sequential soft tissue release and time for soft tissue stretching were anticipated to restore column height. A tricortical graft from the ipsilateral pelvic brim was planned for the 25-millimeter defect, with dorsal spanning plate and volar plate fixation.
Surgical Discussion
Patient positioning: Supine positioning with the arm on a hand table, allowing access for both volar and dorsal approaches.
Anatomical surgical approach: The surgical approach commenced with a volar Henry's approach to the distal radius. Osteotomy and debridement of the malunion site were performed. Distraction was achieved using a threaded pin device between the radial diaphysis and second metacarpal shaft. A dorsal MIPO approach to the third ray was also utilized for minimally invasive insertion of a dorsal spanning plate.
Operative remarks:The surgeon noted that after restoration of joint geometry, a 40 to 50 millimeter segment of tricortical pelvic brim graft was harvested, divided, and impacted along the radial and ulnar cortical columns. The volar aspect was plated with a 2.5 millimeter distal radial T-plate from Aptus. Due to poor bone quality and significant construct tension, this was augmented with an Aptus dorsal spanning plate, secured with three proximal and three distal bicortical locking screws. Removal of the distraction device confirmed retention of reduction.
Postoperative protocol: Postoperative rehabilitation included immobilization with anticipated removal of the dorsal spanning plate in approximately three months.
Follow up: Not specified.
Orthopaedic implants used: 2.5mm Aptus distal radial T-plate, Aptus dorsal spanning plate, 2.5mm threaded pin distraction device. Tricortical pelvic autologus bone graft
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 92 times
27 Mar 2025
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2025). Neglected Intra-Articular Distal Radius Malunion with Ulnar Syndrome. Journal of Orthopaedic Surgery and Traumatology. Case Report 27339089 Published Online Mar 27 2025.