








Terrible Triad Elbow Fracture Dislocation with Radial Head Replacement
Score and Comment on this Case
Clinical Details
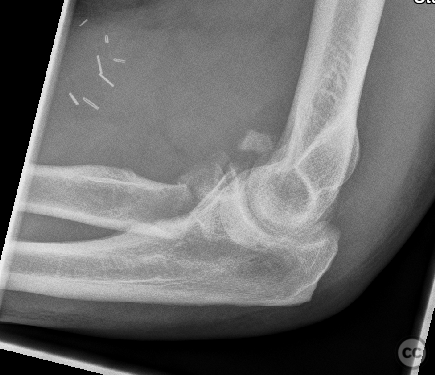
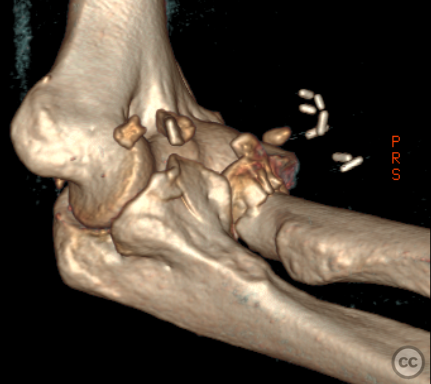
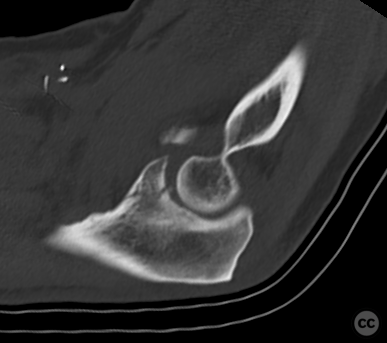
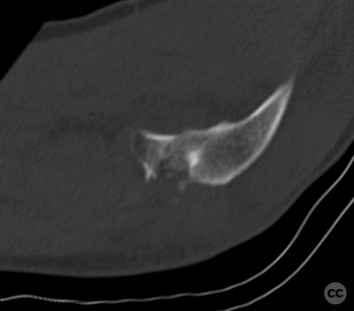
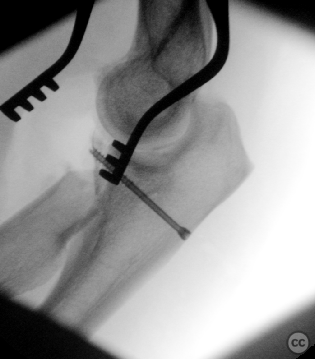
Clinical and radiological findings: A 64-year-old male sustained a motorcycle injury resulting in a terrible triad elbow fracture dislocation, characterized by a multifragmentary Mason IV radial head fracture and a fragmented but mostly nondisplaced coronoid fracture. Initial radiological findings confirmed the complex nature of the injury, with multiple fragments of the radial head and a nondisplaced coronoid fracture. The lateral collateral ligament was avulsed from the lateral aspect of the capitulum.
Preoperative Plan
Planning remarks: The preoperative plan involved a lateral approach to the elbow, centered on an extensor digitorum communis (EDC) split to access the radial head and neck. The plan included resection of the radial head fragments and replacement with a prosthesis, as well as stabilization of the coronoid fracture using a headless compression screw.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table with the left arm placed on an auxiliary table. A tourniquet was applied to the upper aspect of the proximal arm .
Anatomical surgical approach: A curved incision approximately seven centimeters in length was made over the lateral epicondyle of the elbow, extending into the proximal lateral aspect of the forearm. Subcutaneous dissection and hemostasis were performed, followed by an EDC split approach to expose the radial head and neck. The lateral collateral ligament was retracted posteriorly to visualize and remove multiple fragments of the radial head. Resection of the radial neck was performed using an oscillating saw. A stab incision at the posterior aspect of the ulna allowed insertion of a Kirschner wire (K-wire) under fluoroscopic guidance, followed by drilling and placement of a three-millimeter headless compression screw to stabilize the coronoid fracture.
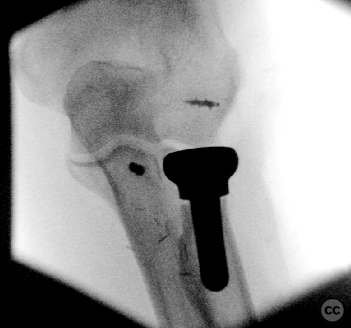
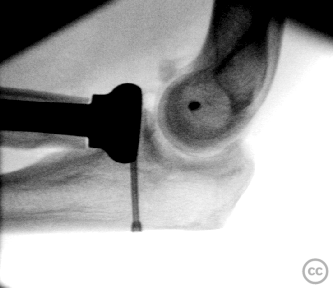
Operative remarks:The radial head was deemed irreparable, necessitating replacement with a prosthesis. Rasping of the proximal radial shaft and trialing with a Zimmer ExploreR shaft and head component ensured appropriate sizing. Final prosthesis implantation was confirmed with fluoroscopy, ensuring optimal joint spacing and stability. A corkscrew titanium anchor was placed at an isometric point on the capitulum for suture refixation of the lateral collateral complex. Range-of-motion testing confirmed stable reduction without subluxation.
Postoperative protocol: Postoperative rehabilitation included unrestricted range-of-motion exercises without immobilization orthosis.
Follow up: Not specified
Orthopaedic implants used: Zimmer ExploreR radial head prosthesis, 3mm headless compression screw, Kirschner wire, Arthrex corkscrew titanium anchor
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 248 times
17 Jul 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Terrible Triad Elbow Fracture Dislocation with Radial Head Replacement. Journal of Orthopaedic Surgery and Traumatology. Case Report 30306534 Published Online Jul 17 2024.