











Complex Monteggia-like fracture dislocation with coronoid deficiency
Score and Comment on this Case
Clinical Details
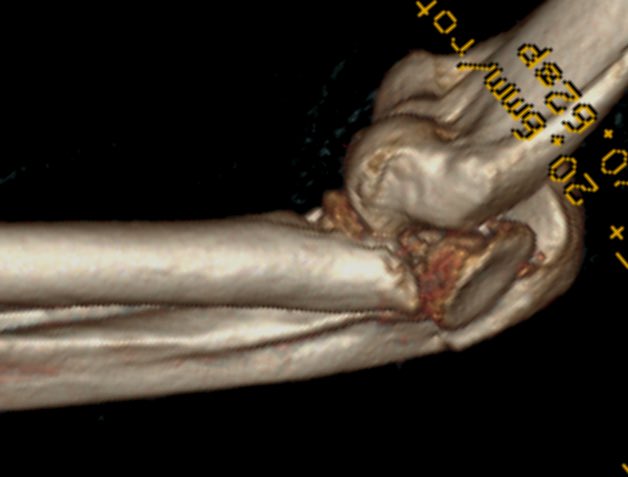
Clinical and radiological findings: This case represents a complex Monteggia like fracture-dislocation in a 40-something year old male following fall from a height of over 3 m. Preliminary plain film imaging demonstrates a posteriorly dislocated elbow joint with complex fracture pattern of the proximal ulna together with a grossly displaced fracture dislocation of the radial head and neck. Superficial soft tissue abrasions and contusion around the olecranon but to the fracture was still considered closed. Due to soft tissue concerns the arm was initially immobilised and an external fixator and definitive fixation occurred in the 10 to 14 day time window. In this time a preoperative CT allowed planning of the reconstruction and it the ordering of necessary implants. Special consideration was given to the reconstruction of the coronoid which appeared completely submarined under the trochlea and was no longer identifiable as a discrete fragment.
Preoperative Plan
Planning remarks:
Surgical Discussion
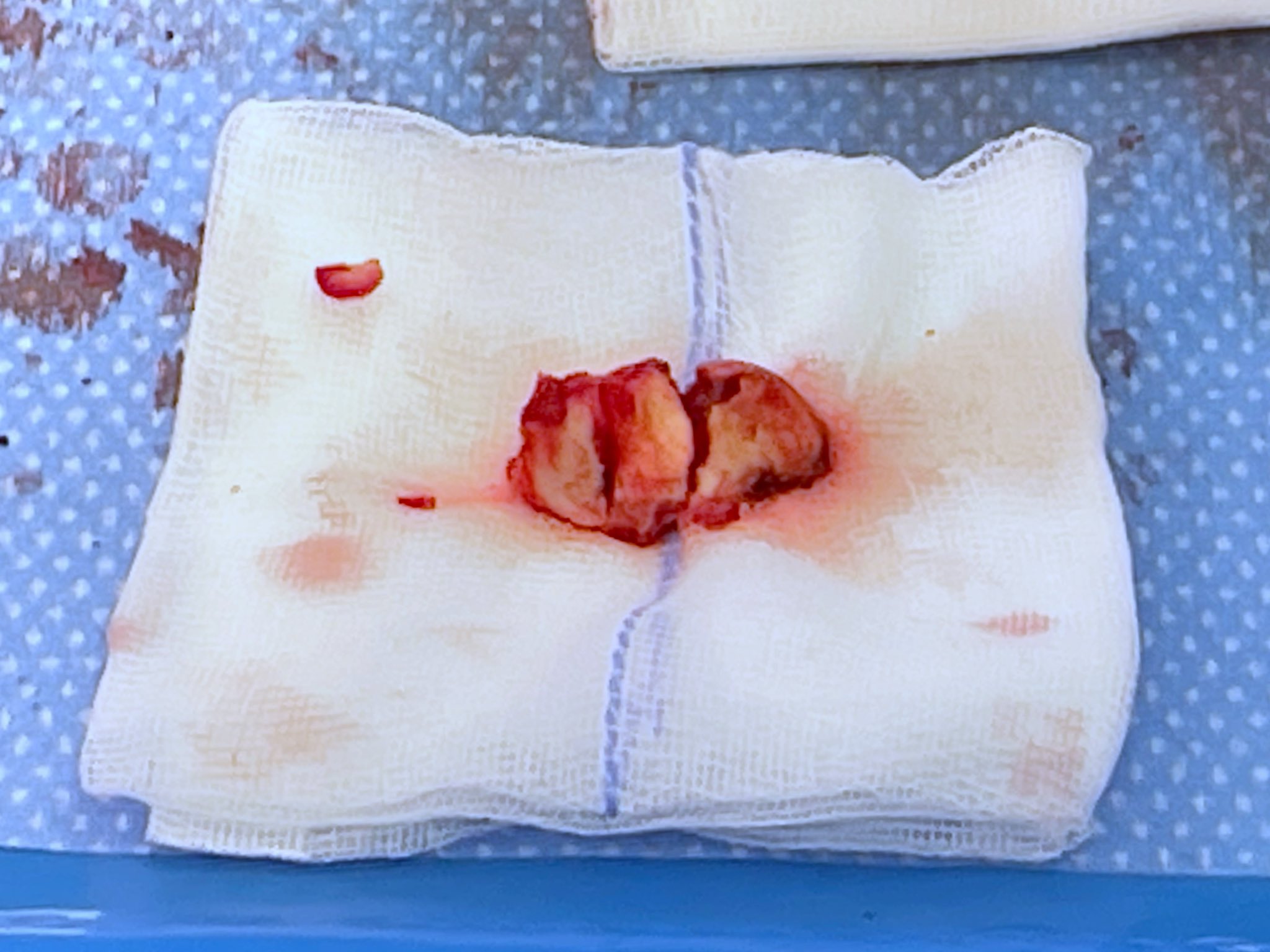
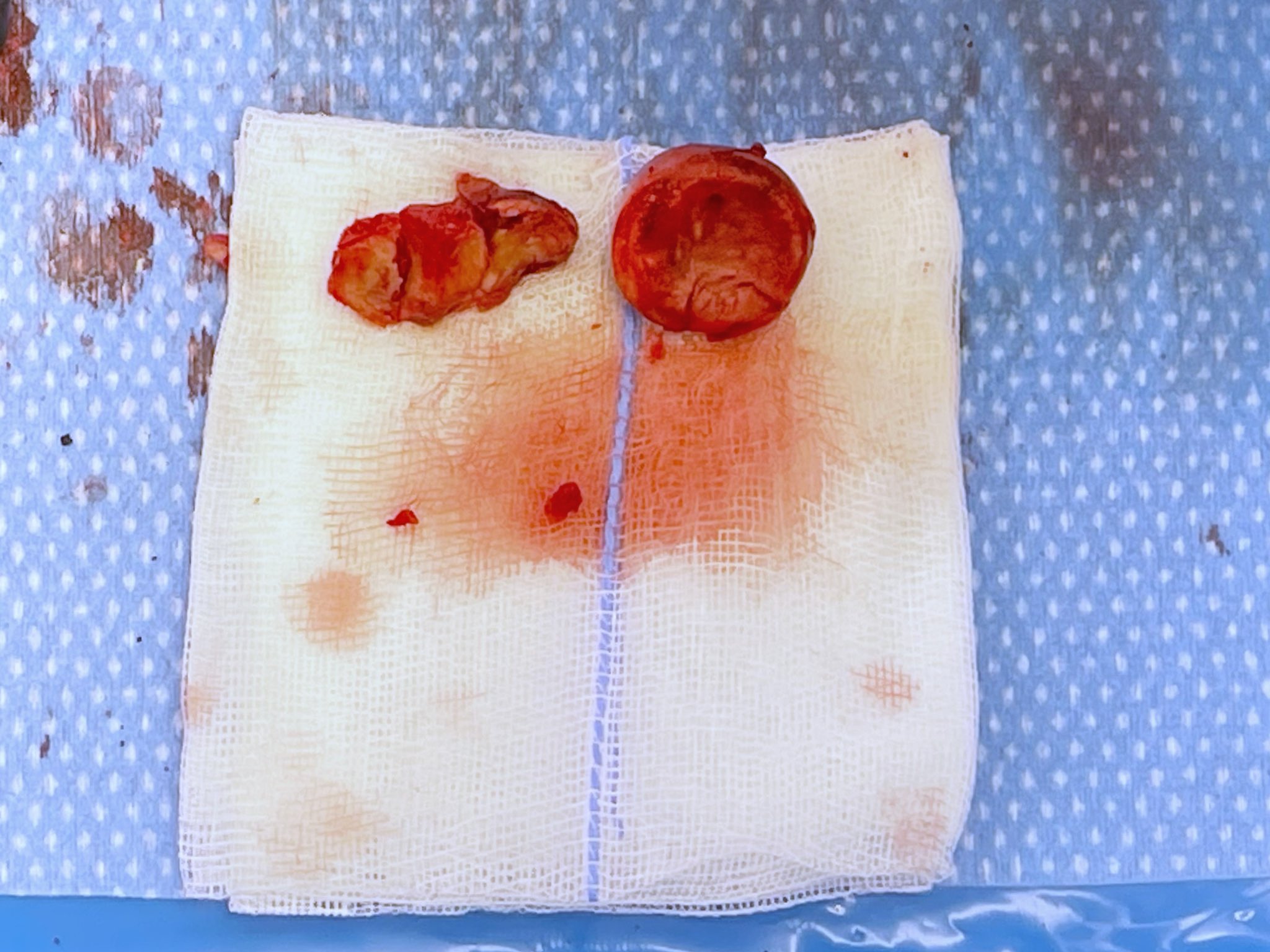
Operative remarks:The operation was done supine with the arm flexed at the elbow and rested on an arm support placed above the patients chest. The surgical approach was primarily through Boyd's interval through which reduction of the joint and retrieval of bony fragments was possible. Consistent with preoperative planning it was decided early to sacrifice the radial head and neck which was resected to stable bone. Removal of the radius allowed good visualisation of the coronoid, or rather the location where the coronoid should be. Through this window in combination with a limited Taylor Shamm approach we could stabilise the ulna and olecranon as a single functioning unit. 3 individual fragments were retrieved from the joint which ultimately represented the coronoid. These pieces were reconstructed on the back table using inter fragmentary k wires which were then reintrotuced and reduced into position through an FCU split approach to the medial side. The bony defect anterior to the coronoid process was filled with radial head autograph which provided a buttress to the the articular coronoid fragments. This conglomeration of fragments was then fixed with both a coronoid plate from aptus, together with a poster anterior lag screw wedging the radial head graft into place. Dynamic stability testing under fluoroscopy demonstrated congruent and stable joint two within 10 degrees of full extension. The patient has been lost to follow-up in the post-operative period. I will be trying to contact him in the near future to assess his mid-term clinical outcome.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 678 times
23 May 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Complex Monteggia-like fracture dislocation with coronoid deficiency. Journal of Orthopaedic Surgery and Traumatology. Case Report 30958433 Published Online May 23 2022.