


















Hardware Failure of Primary Gamma Nail Osteosynthesis in Transtrochanteric Femoral Fracture
Score and Comment on this Case
Clinical Details
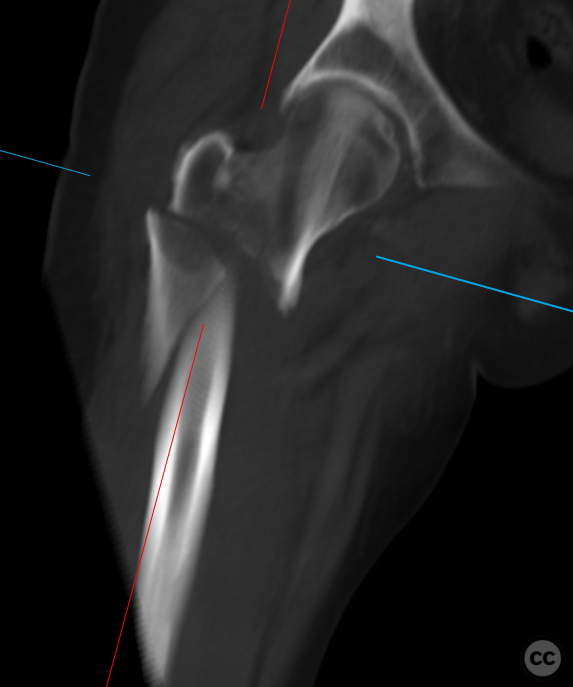
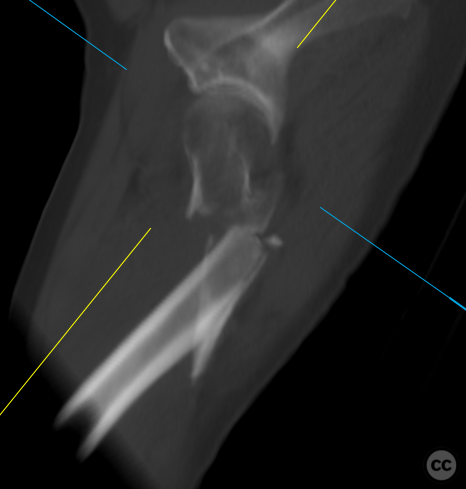
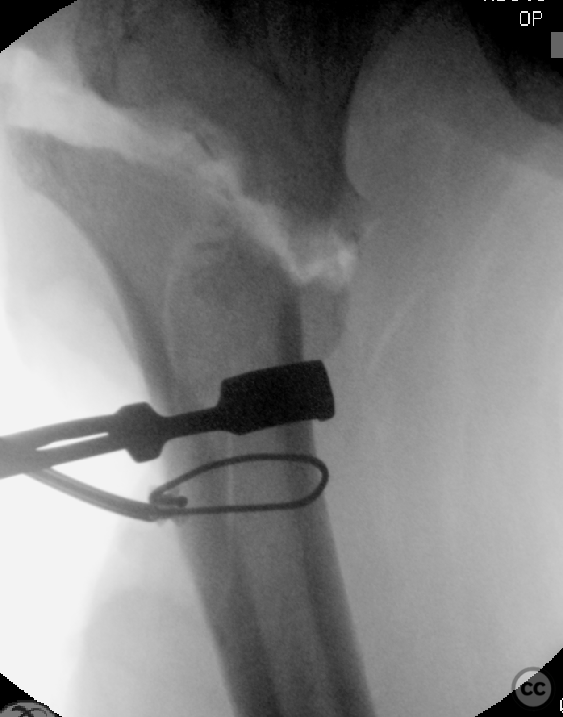
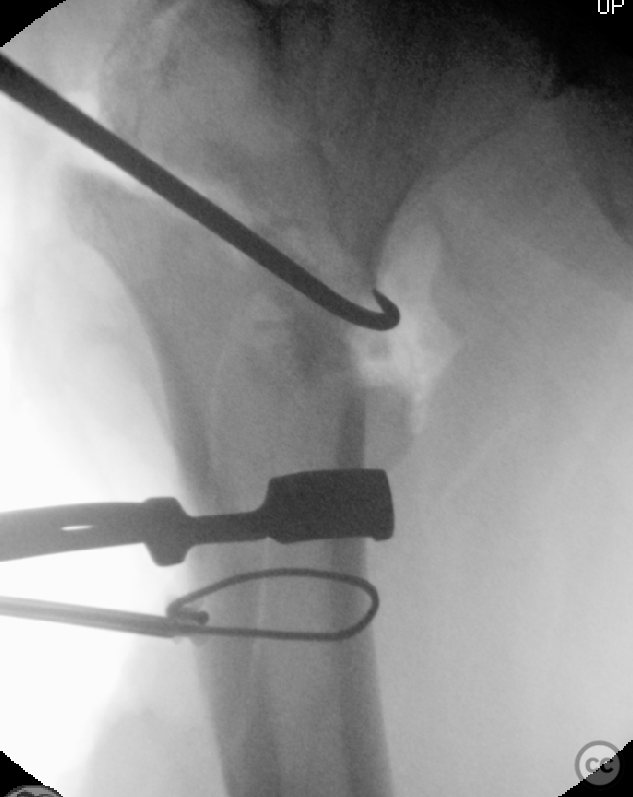
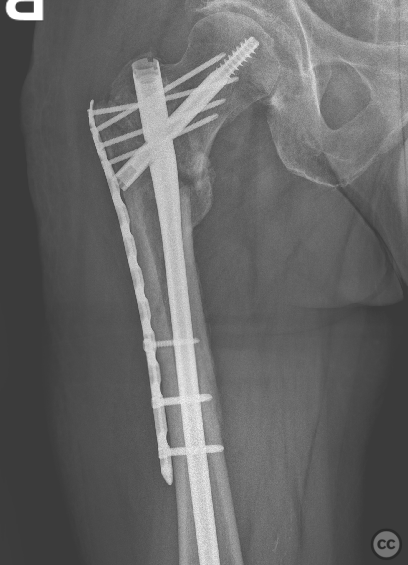
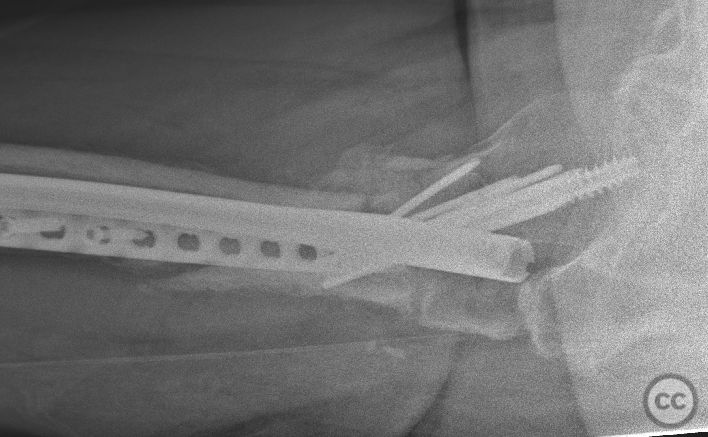
Clinical and radiological findings: A 56-year-old male experienced an industrial fall from a height of 3-5 meters, resulting in an isolated lower extremity injury. Neurovascular status was intact, and the injury was closed. The patient was a large and heavy-set individual. Initial trauma CT diagnotic revealed a transtrochanteric femoral fracture with a further long lateral wall fragment. The initial operative management by the on-call team included open reduction and cerclage fixation of the lateral wall, together with open clamp reduction of the proximal fracture fragment, followed by the introduction of a Gamma3 cephalomedullary nail. This initial approach achieved near anatomic fracture reduction and alignment without any appreciable varus nor significant rotational malreduction. The patient was managed FWB in the post operative period, and the inital XRs following ambulation demonstrated satisfactory retention of reduction. At 5 weeks post-operation, the patient presented with sudden atraumtaic pain and inability to bear weight, indicative of hardware failure. Imaging showed varus collapse and nail failure at the screw/nail junction.
Preoperative Plan
Planning remarks: The revision aimed to remove the broken nail and cerclage wire, and address the biomechanical situation the had resulted in failed hardware: Consideration was given to changing to a recon type nail, however given the satisfactory existing screw position, plus the availability of some additional dept to reseat a new screw, the plan was to introduce a new Gamma CMN with an additional lateral tension plate to provide varus stress relief to the nail. Additionaly, the postoperative weightbearing status would be modified pending bony union.
Surgical Discussion
Patient positioning: Supine on a traction table
Anatomical surgical approach: Lateral utility approach through the old wound, then a combined Watson-Jones approach was utilized for access to the hip and ventral pertrochanteric region, combined with trans and sub-vastus approaches to the proximal femoral shaft
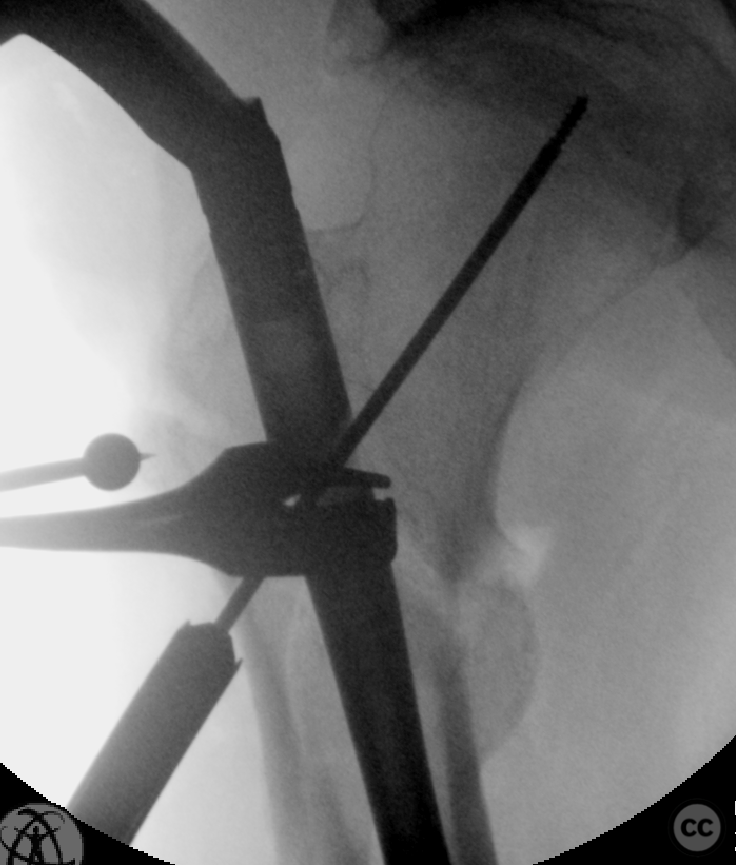
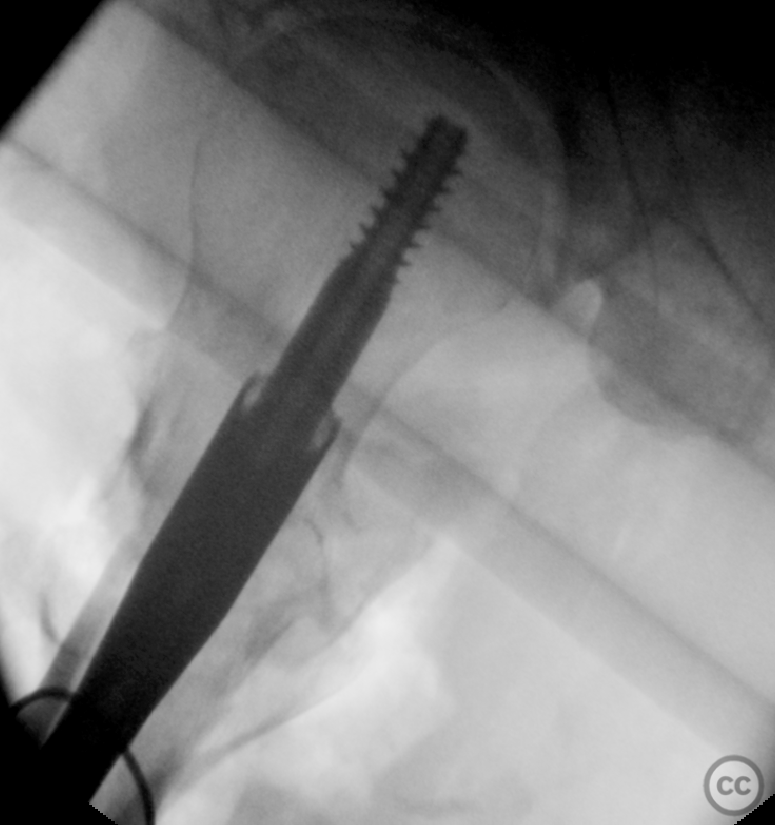
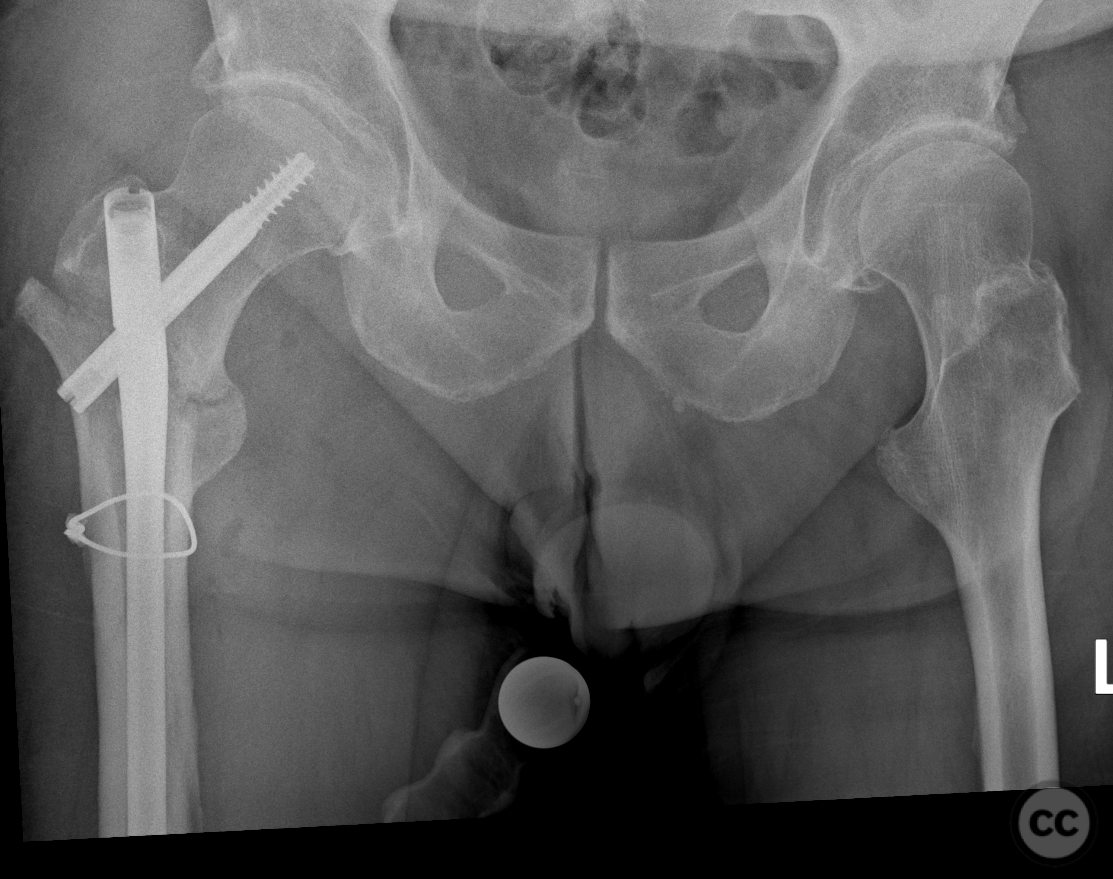
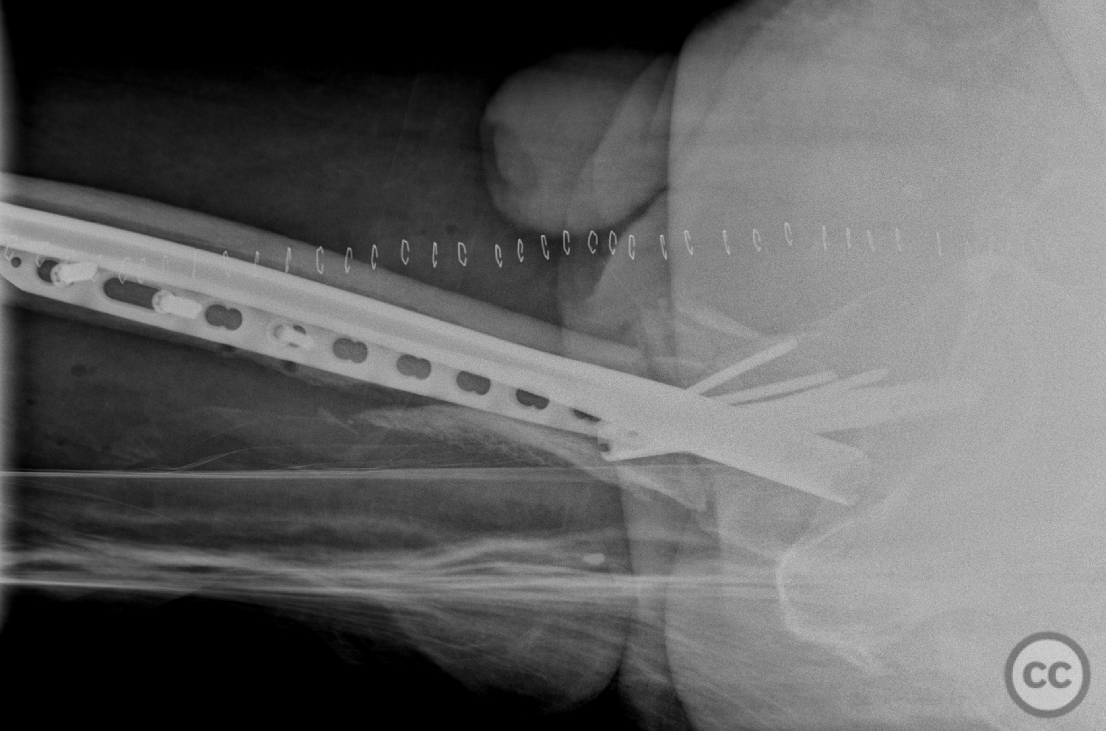
Operative remarks:Removal of the failed hardware, debridement of callus, and difficult re-reduction due to soft tissue scarring and existing callus. A revised fixed-angle construct was assembled, this time dynamically compressed intraoperatively ensuring engagement of the medial column. Additionally I incorporated a lateral tension plate designed to counter varus torque and stress-relieve the CMN at the site of previous failure (the nail/screw interface).
Postoperative protocol: Postoperative rehabilitation protocol included 20kg touch-weight bearing for 4 weeks, followed by 50% weight bearing for another 4 weeks before progressing to full weight bearing, adjusted according to follow-up radiology.
Follow up: Not specified
Orthopaedic implants used: Stryker Gamma3 cephalomedullary nail, 3.5/4.5 Synthes metaphyseal plate as lateral tension plate.
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 2472 times
19 Mar 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Hardware Failure of Primary Gamma Nail Osteosynthesis in Transtrochanteric Femoral Fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 31189582 Published Online Mar 19 2024.