







Terrible triad injury of the elbow - radial head reconstruction and LCL stabilization
Score and Comment on this Case
Clinical Details
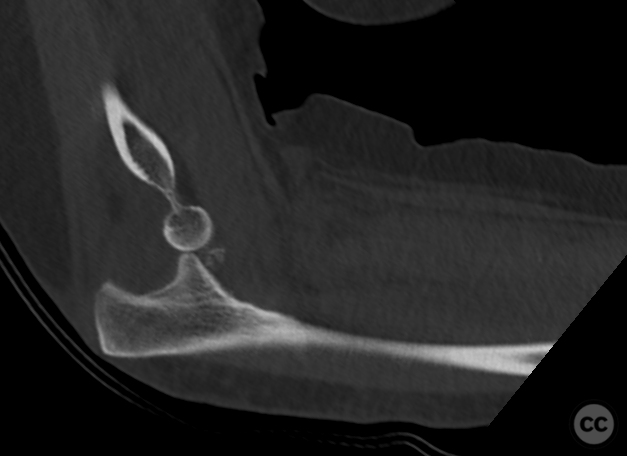
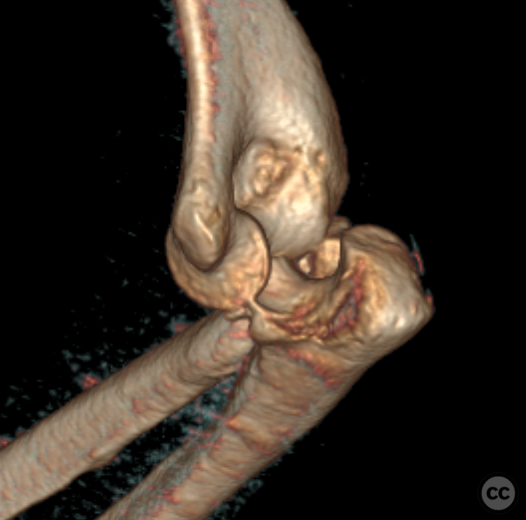
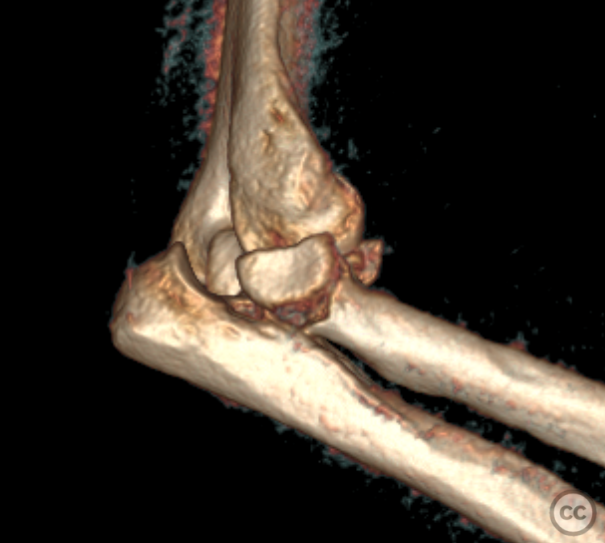
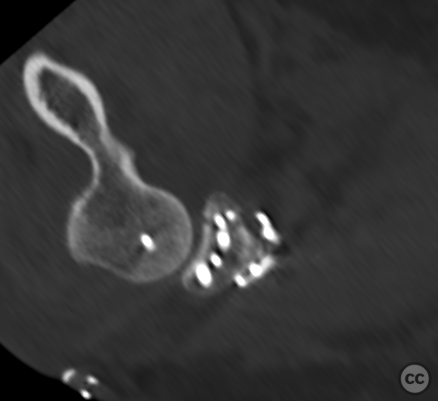
Clinical and radiological findings: An 80-year-old female experienced a ground-level fall at home, resulting in a posterolateral dislocation of the right elbow, a multifragmentary displaced radial head fracture (Mason IV), and a type I coronoid fracture. Initial management included closed reduction and splinting; however, due to other injuries requiring surgical intervention and the insufficiency of the splint to maintain reduction, an external fixator was applied on day 2. By day 6, soft tissue conditions were deemed suitable for definitive fixation.
Preoperative Plan
Planning remarks: The surgical plan entailed radial column repair focusing on the radial head and lateral collateral ligament (LCL) stabilization. Open reduction and internal fixation (ORIF) were planned with a backup option for radial head replacement if necessary.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table, with the right arm crossed over the chest on a secondary arm support to achieve 90 degrees of elbow flexion. The external fixator was removed, followed by surgical site preparation.
Anatomical surgical approach: A dorsal incision was made over the proximal ulna, curving around the olecranon tip, incorporating the external fixator pin sites for excision and secondary closure. Subcutaneous dissection exposed the anconeus muscle along the radial aspect of the ulna. A capsulotomy extended around the olecranon apex, allowing identification of the lateral ulnar collateral ligament and its insertion on the supinator crest. Sharp dissection facilitated elevation of supinator muscle fibers for radial neck and head fracture exposure.
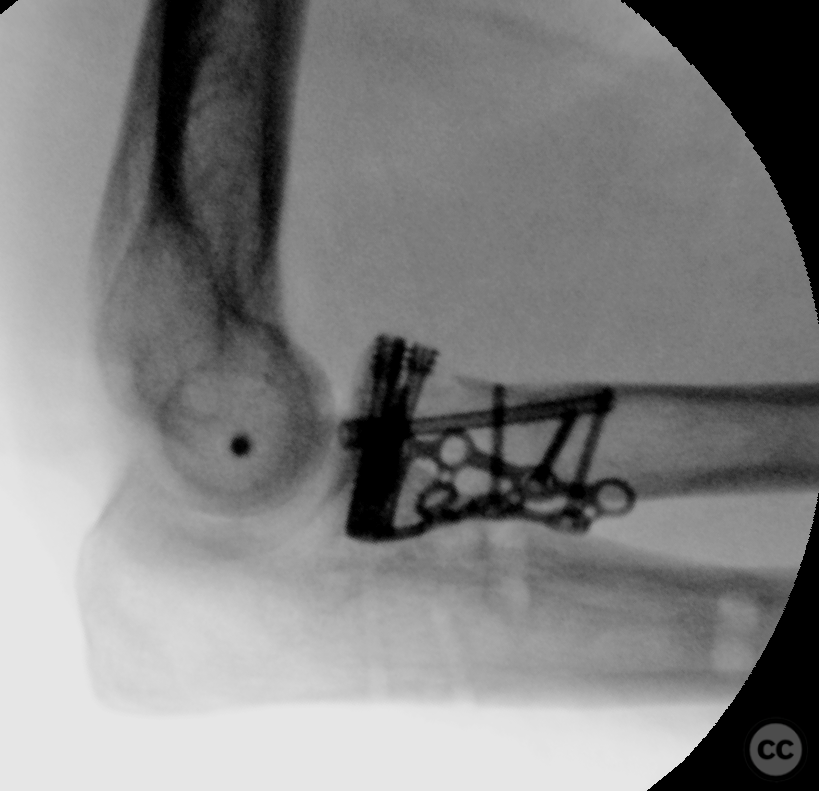
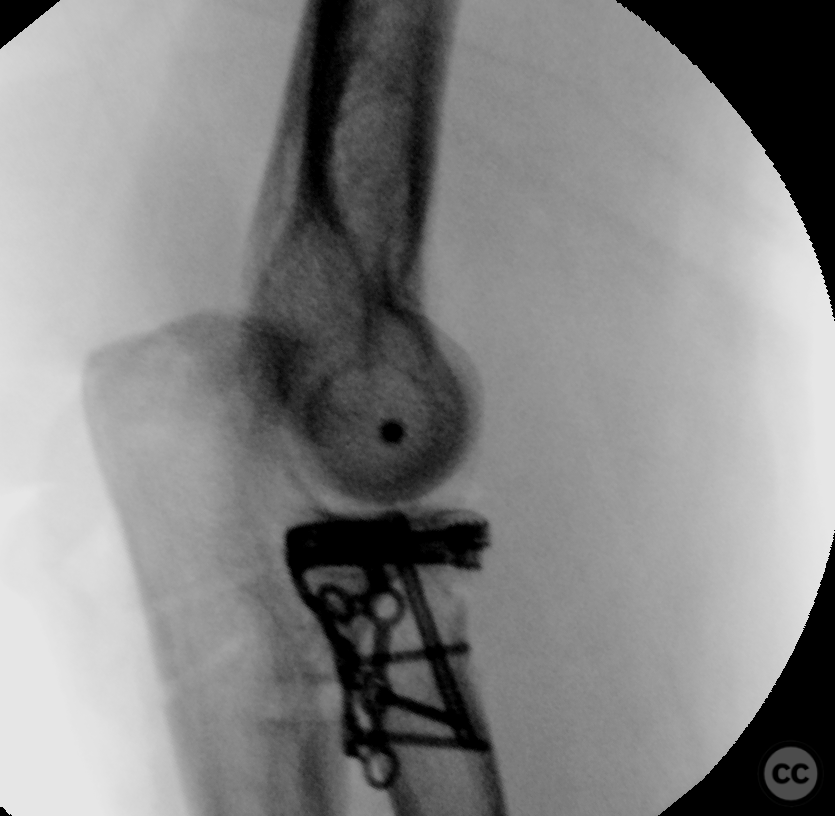
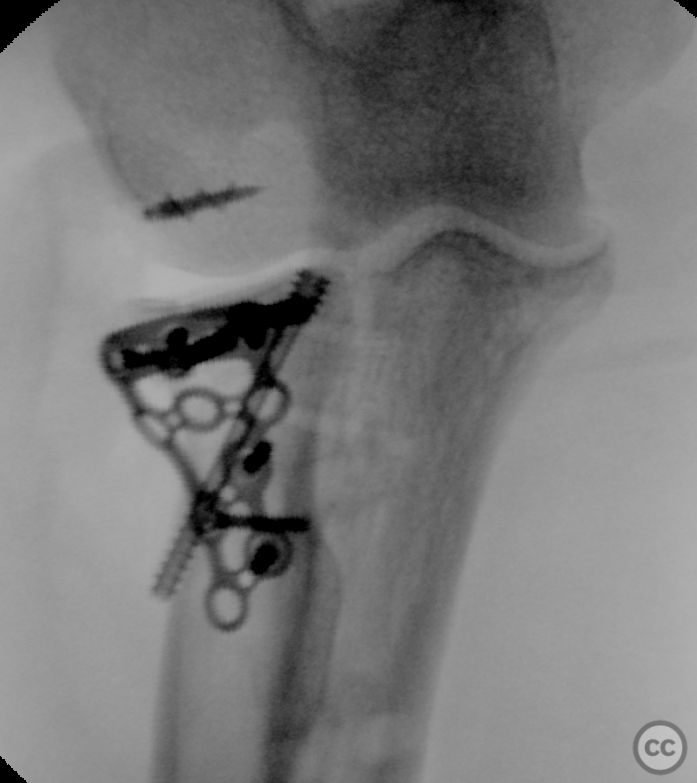
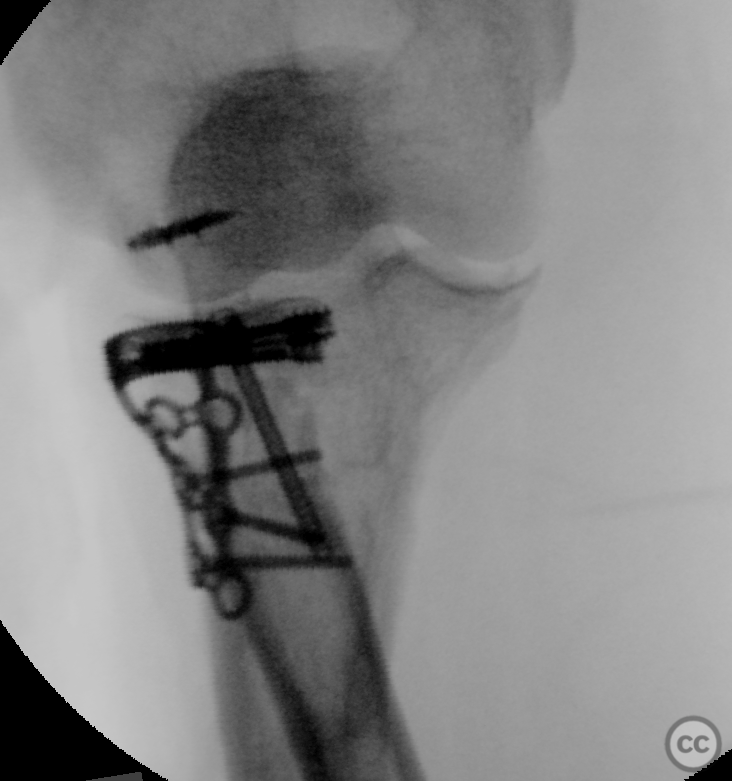
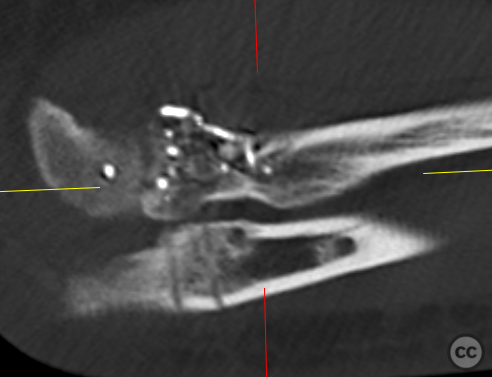
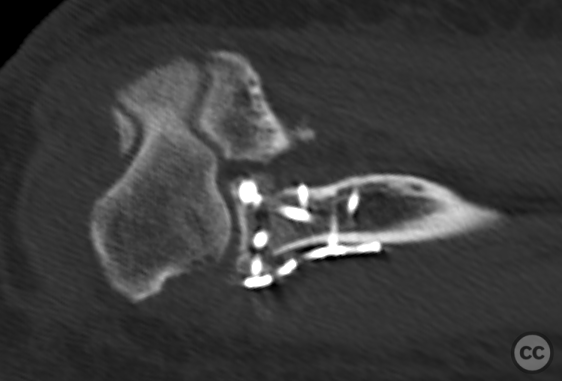
Operative remarks:Intraoperatively, multiple small osteochondral fragments were removed, and two large radial head fragments were identified, reduced on the back table where they were provisionally fixed with K-wires followed by HBS screws.
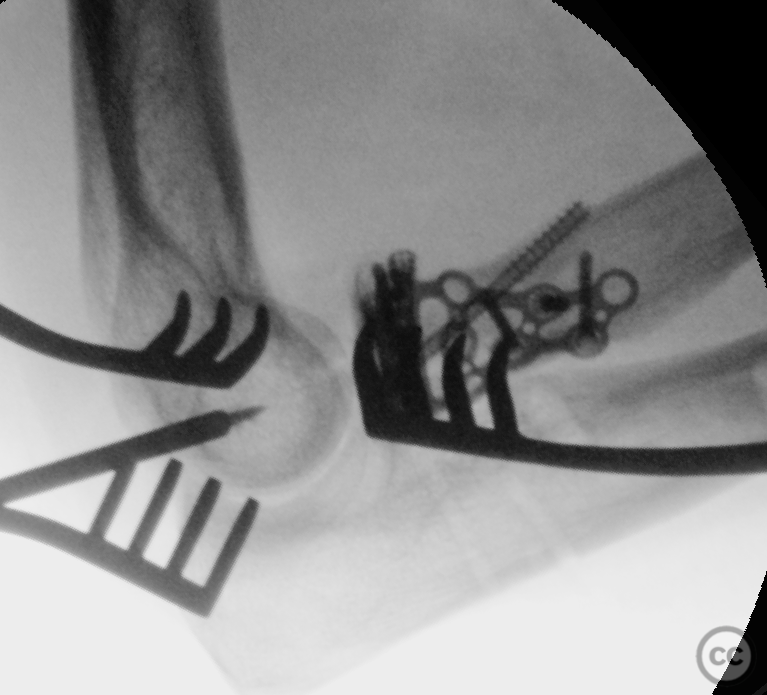
The radial head was then anatomically reduced to the neck (based on morphology of the PRUJ articular surfec - in the absence of any other fracture landmarks) with K-wire fixation before securing with a 2.0 mm Aptus proximal radial rim plate and locking screws. An oblique antegrade screw provided additional support.
The LCL was reattached to the supinator crest using FiberWire through transosseous tunnels. A lateral EDC split approach revealed a humeral-sided avulsion of the LCL complex, which was repaired with a 3.5mm titanium corkscrew anchor and FiberWire.
Postoperative protocol: Postoperative rehabilitation encouraged early non-weight-bearing range of motion from day one without immobilization.
Follow up: Not specified.
Orthopaedic implants used: HBS midi screws, 2.0 mm Aptus proximal radial rim plate, 1.0 mm K-wires, Arthrex 3.5 mm titanium corkscrew anchor preloaded with FiberWire.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
User Discussion (1)
Guest User
Is that not a lot of hardware in the radial head?