
Proximal hamstring tendon avulsion
Score and Comment on this Case
Clinical Details
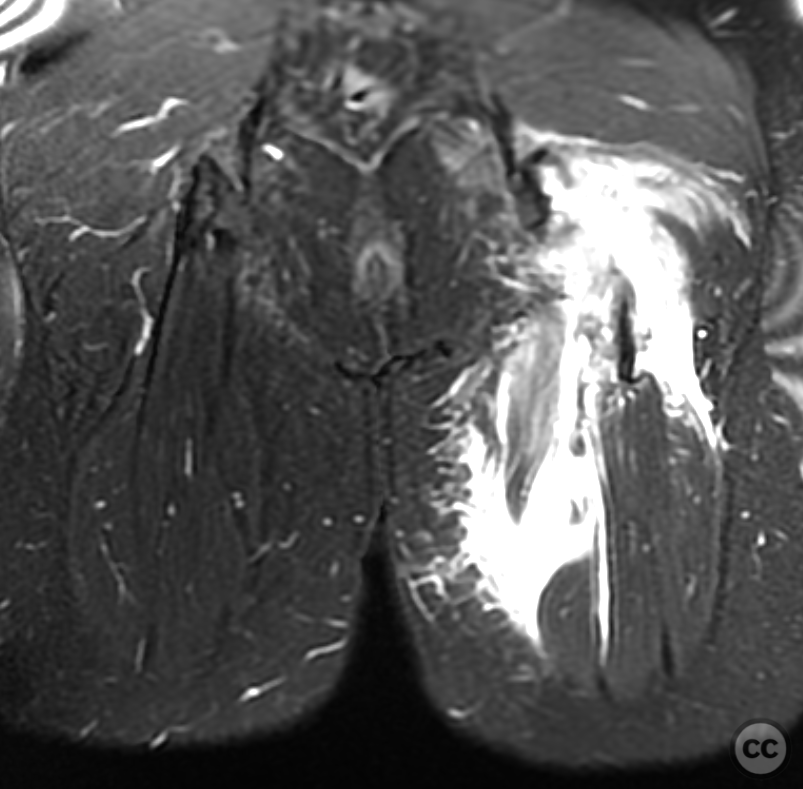
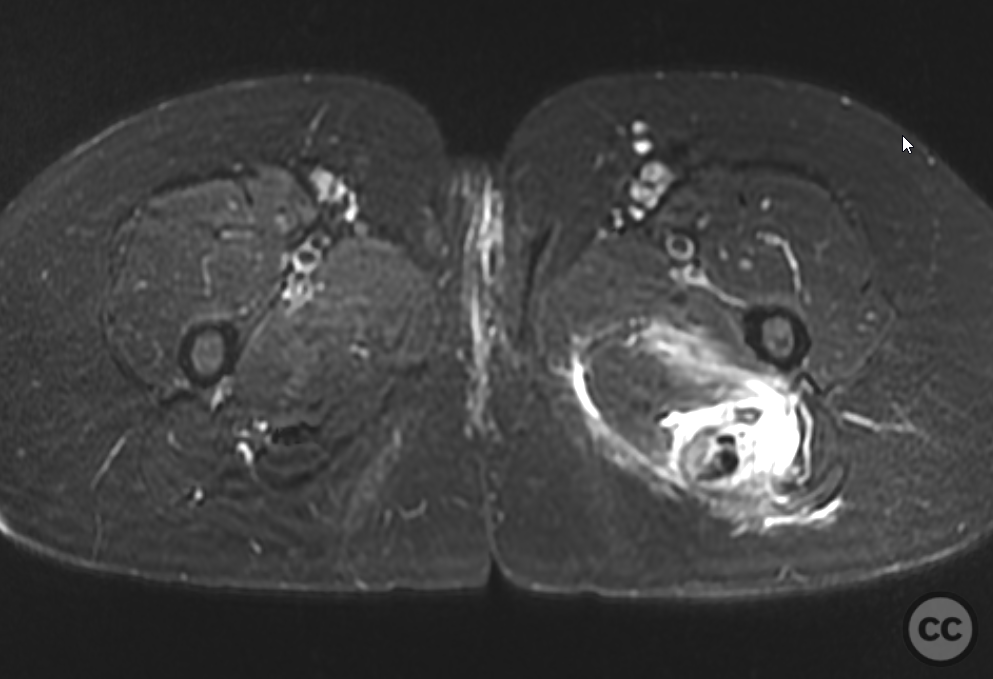
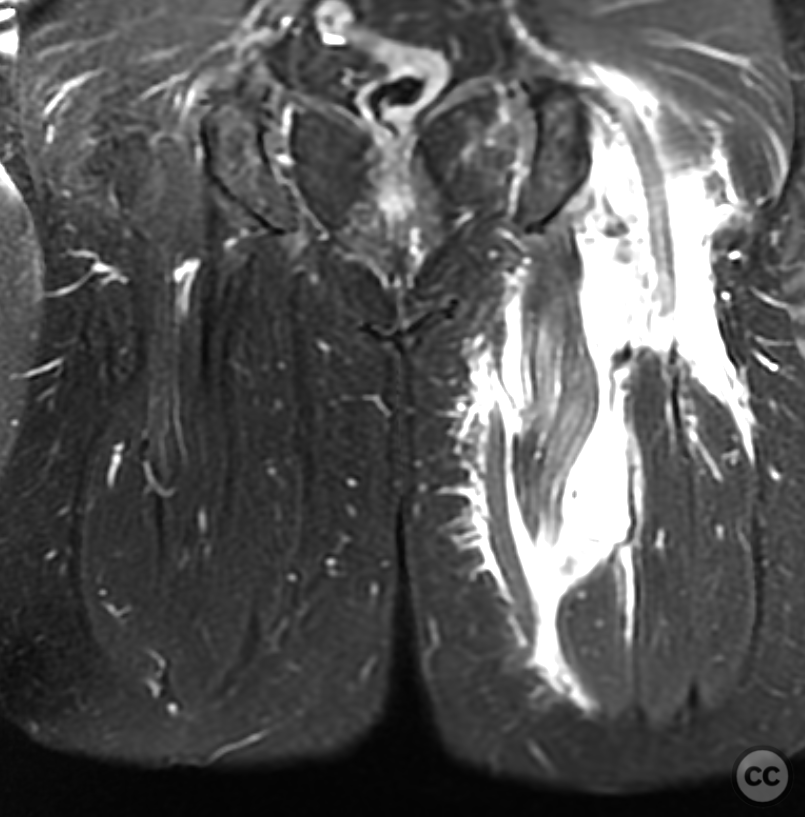
Clinical and radiological findings: This case is a female manual worker in her mid-40s who sustained an awkward standing height fall with hyperflexion of the hip and forced extension of the knee resulting in a proximal hamstring avulsion. A workers comp injury claim the patient was highly motivated for a rapid return to work. The MRI images provided we're obtained relatively acutely and the delay to surgery was well under 14 days. There is certainly some controversy regarding surgical fixation of this injury. Good results can be achieved through conservative management. The literature does however support the idea of accelerated rehab and early return to function in surgically managed patients. The clinical outcomes of surgical management can be better than conservative management in select patient populations. Some literature is provided at the end for review.
Preoperative Plan
Planning remarks:
Surgical Discussion
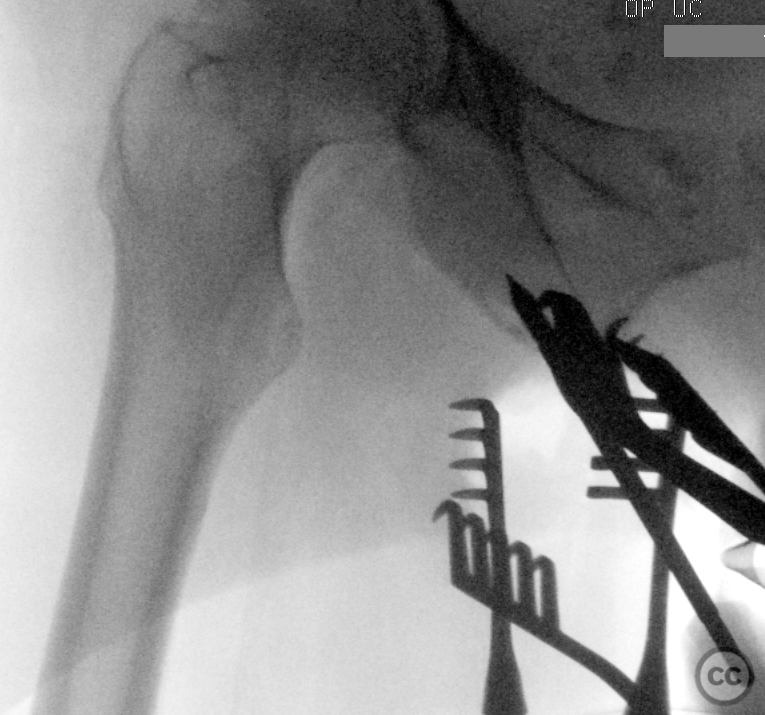
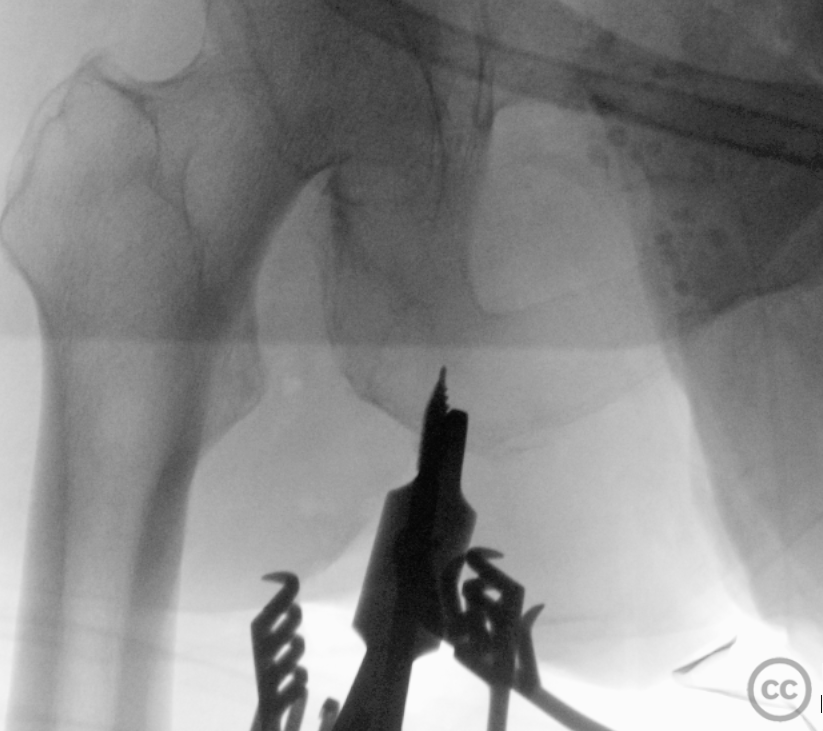
Operative remarks:This case was done prone on a radio translucent operating table. The hip was in neutral extension and the knee was flexedto around 45 degrees of flexion. Given the level of retraction of the tendon in MRI and the relative short delay to surgery a limited transverse incision on the medial aspect of the gluteal fold was done. Incision was limited to around 6 cm. Blunt subcutaneous dissection and then longitudinal incision of the muscle fascia provided direct access to the tendons stumps which were both directly visualized and easily mobilised digitally in the wound. The course of the sciatic nerve is immediately deep and lateral to the zone of injury. It could be palpated deep in the wound base. A direct visualisation of the nerve was not necessary. The tendons were debrided and whip stitched with suture tape resulting in a 4 strand whipstitch construct. Retraction of of the gluteal musculature proximally demonstrated the ischial tuberosity and some residual hamstring remanants still attached at their bony origin. Limited sharp debridement of the footprint was performed followed by placement of two K Wires in the approximate location of the the desired anchors. The location of both wires was confirmed radiologically in orthogonal planes. Following confirmation of anchor positioning the wires were removed and replaced with two 5.5 mm bioabsorbable anchors in which the fibre tapes were loaded. Final tying down of the fibre tapes resulted in excellent adaptation of the stumps to bone. Only moderate tension of the reduced hamstrings was evident with 45 degrees of knee flexion. Knee extension to 30 degrees increased tension without compromising anchor fixation. Post-operative management of this patient will not be particularly restrictive. 90 degree hip flexion is to be limited and in coordination with 90 degree knee flexion. Hip flexion with extended knee is to be avoided until 10 to 12 weeks postoperatively.
Orthopaedic implants used: Arthrex biocomposite corkscrew suture anchors
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 946 times
28 Dec 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Proximal hamstring tendon avulsion. Journal of Orthopaedic Surgery and Traumatology. Case Report 32046389 Published Online Dec 28 2022.