




Maisonneuve Fracture with AITFL rupture
Score and Comment on this Case
Clinical Details
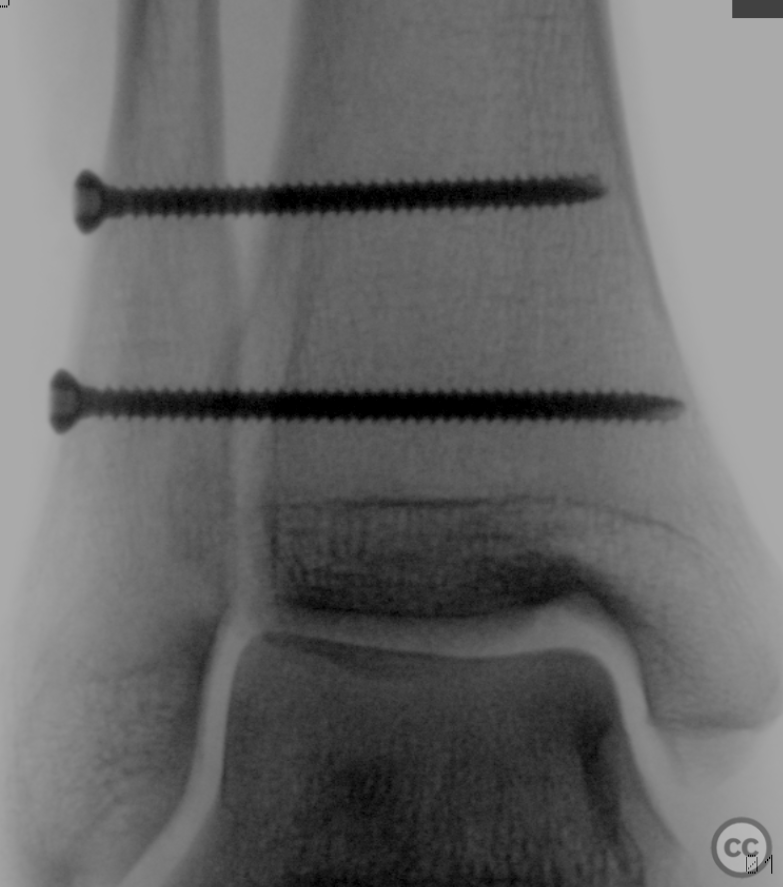
Clinical and radiological findings: A 55-year-old male presented following a simple twist and fall injury. Initial plain radiographs revealed a fracture of the proximal fibula. Ankle radiographs showed no diastasis, although stress films were not performed. Clinical examination was unremarkable for neurovascular compromise.
Preoperative Plan
Planning remarks: The preoperative plan involved surgical exploration of the ventral syndesmosis to assess the extent of ligamentous injury. The reduction of the fibula was planned using the "Mercedes sign" for congruency assessment between the tibia, talus, and fibula. Fixation of the tibiofibula joint was planned with syndesmotic screws.
Surgical Discussion
Patient positioning: Supine position on a radiolucent table, wedge under the ipsilateral hemipelvis
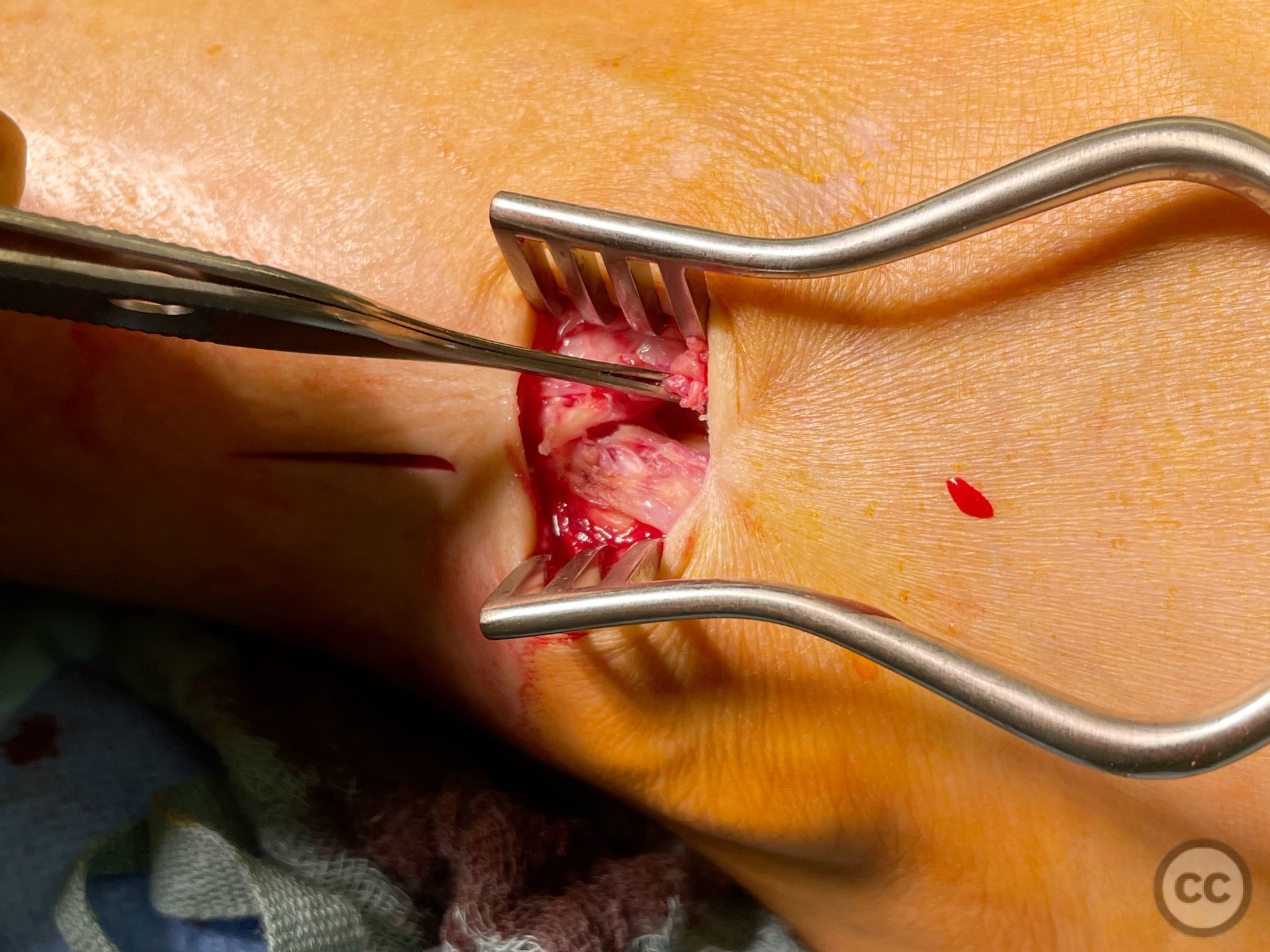
Anatomical surgical approach: A limited 2 window lateral approach to the distal fibula was utilized. distally based over the syndesmosis, and proximally more lateral for minimally invasive screw insertion.
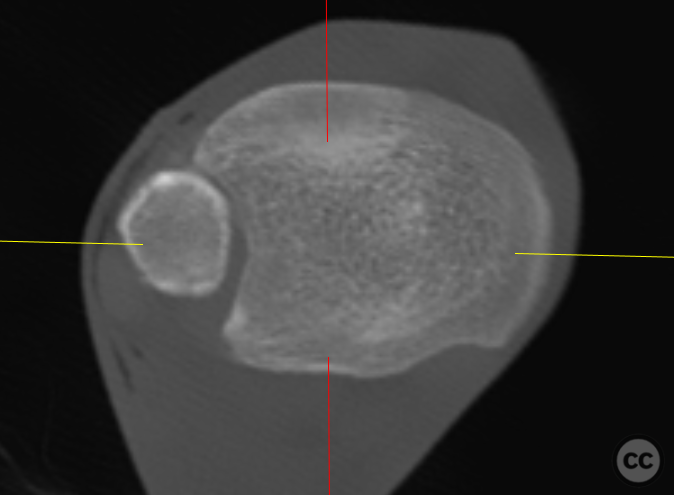
Operative remarks:Intraoperative findings confirmed a complete rupture of the ventral syndesmosis (see intraop images). The fibula was reduced using the Mercedes sign, confirming fibular congruency with the tibia and talus. Two syndesmotic screws were placed to stabilize the ligamental repair. Intraoperative 3D imaging confirmed satisfactory reduction and appropriate hardware placement.
Postoperative protocol: Postoperative protocol included non-weight bearing for 6 weeks, followed by progressive weight bearing as tolerated. Range of motion exercises were initiated early to prevent stiffness.
Follow up: Not specified.
Orthopaedic implants used: Two syndesmotic screws.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
User Discussion (1)
Guest User
Don’t you put this screws over a 1/3 tubular? Nice branch waiting for haunting you
It was me the previous comment,strangely doesn’t login