








Segmental humerus fracture - Helix PHILOS plate technique
Score and Comment on this Case
Clinical Details
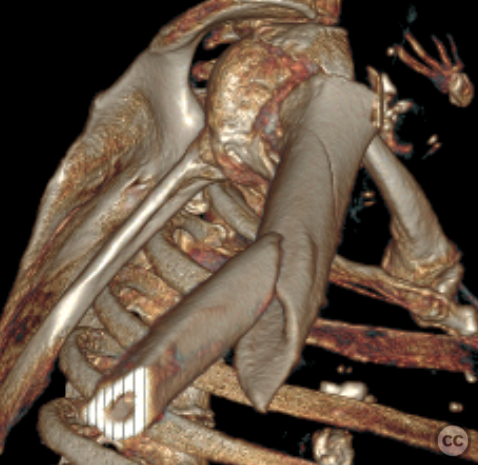
Clinical and radiological findings: atient who presented to the emergency department following a mechanical ground-level fall. The patient, characterized by notable corpulence, sustained a closed injury with preserved neurovascular integrity. Plain radiographic imaging revealed a segmental subcapital and a segmental spiral fracture of the right humeral shaft, with the distal spiral fracture exhibiting over 100% displacement. Due to the patient's body habitus, conservative treatment was deemed unlikely to succeed. After extensive discussions with the patient, we opted for osteosynthetic stabilization. A pre-operative CT was conducted, which highlighted the complexity of the surgical neck fracture, including a proximal spiral component and a small, non-displaced butterfly fragment. Additionally, a secondary spiral fracture was noted in the mid to distal third of the humerus, accompanied by a displaced butterfly segment in the mid-shaft region.
Preoperative Plan
Planning remarks: In planning the surgical approach, both nailing and plating techniques were evaluated. However, due to the comminution surrounding the surgical neck and concerns regarding adequate head fixation, we decided to proceed with a plate for osteosynthesis.
Surgical Discussion
Patient positioning: Semi beach chair
Anatomical surgical approach: Deltopectoral merging into an aggregate anterior approach
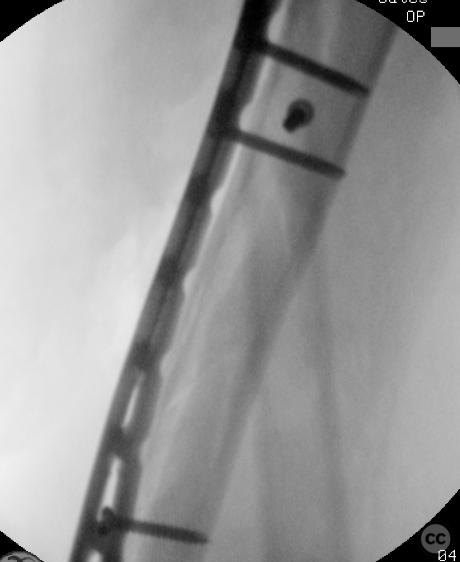
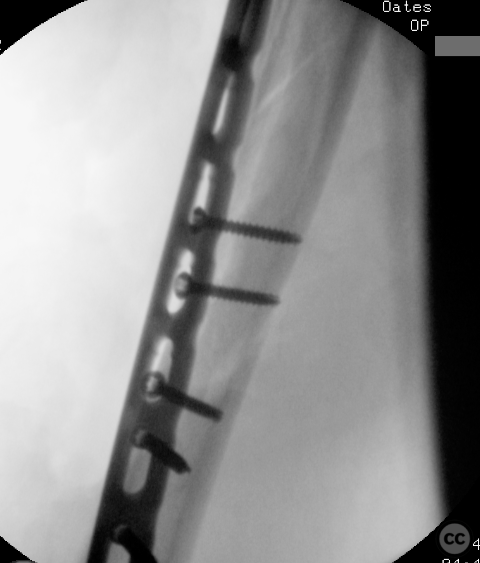
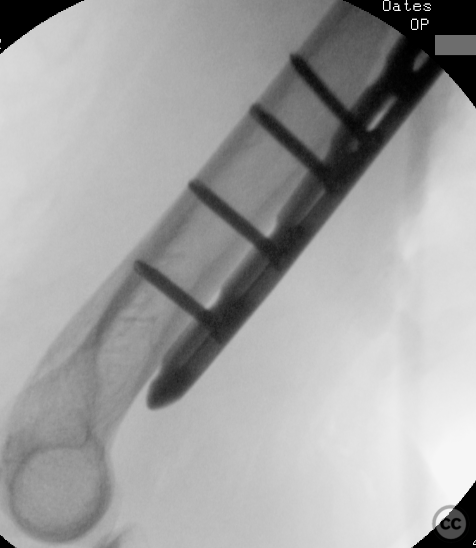
Operative remarks:The patient was positioned in a semi-beach chair configuration, and the right arm was secured in a spider pneumatic arm holder. Extended deltopectoral incision transitioning into an anterolateral approach distally. During surgery, we dissected through the deltopectoral interval, identifying the lateral border of the biceps and the transition of the deltoid insertion into the proximal brachialis musculature. Through blunt dissection bezween muscle bellies, we visualized the multiple butterfly fragments without detaching significant muscle mass. We utilized three fragment-specific 3.5 mm bicortical lag screws to secure the butterfly fragments. Given the anatomical relationship of one large spiral fragment to the deltoid insertion, we opted against releasing it. Instead, a posterior blunt dissection posterior to deltoid created a window from the proximolateral humeral head, continuing posterior and deep to deltoid, and emerging anterolaterally between the medial and lateral heads of the brachialis. A limited release of the lateral head of the brachialis was necessary to accommodate the placement of a 268 mm Philos plate, which was contoured and positioned along this subdeltoid posterio position. Multi-planar fluoroscopy was employed to confirm the provisional positioning of the plate prior to fixation with two bicortical 3.5 mm screws at both proximal and distal aspects. Á total of six proximal monocortical screws in the humeral head, along with two bicortical locking screws in the proximal diaphysis and three bicortical distal locking screws in the distal humeral diaphysis, resulted in a robust bridge plate construct. There was no visualisation of the radial nerve in either the proximal or distal approach windows locations.
Postoperative protocol: Free ROM
Orthopaedic implants used: 268mm Philos - Helix Bend. Note the imaged Phios plate is from a previous case, and does not represnt the over 90deg of twist required in the current case
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 387 times
19 Nov 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Segmental humerus fracture - Helix PHILOS plate technique. Journal of Orthopaedic Surgery and Traumatology. Case Report 32908155 Published Online Nov 19 2024.