








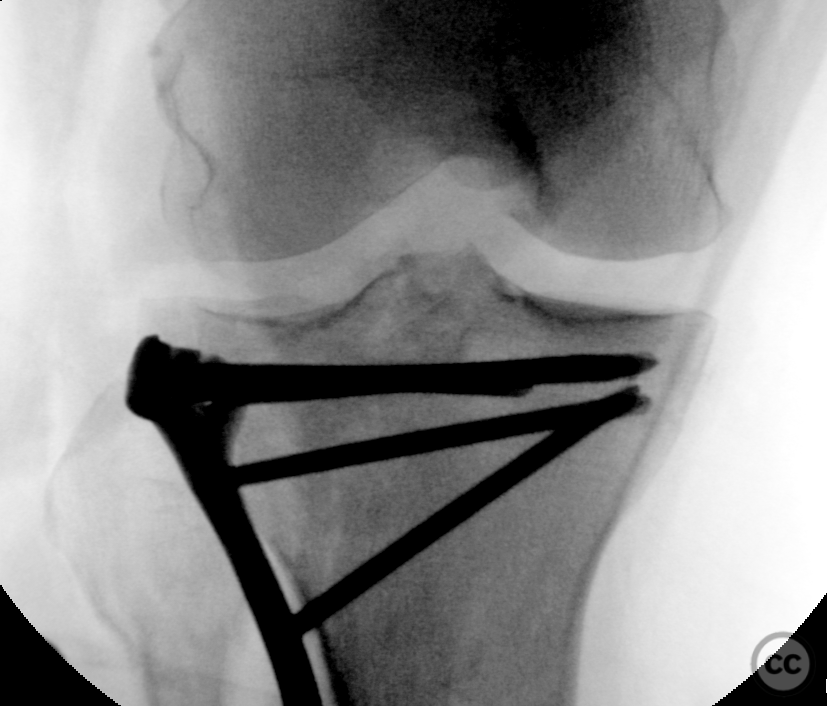

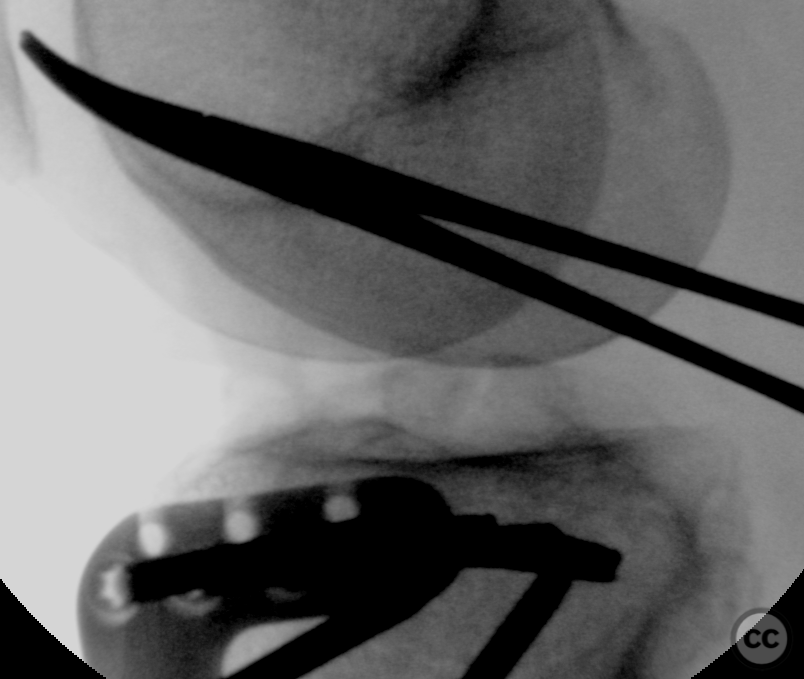
Schatzker II split depression with complete meniscocapsular separation
Score and Comment on this Case
Clinical Details
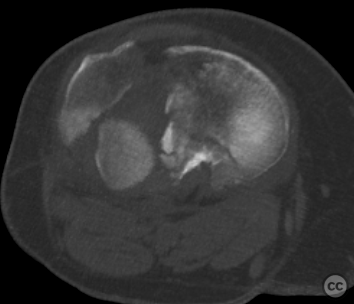
Clinical and radiological findings: 66yo F who sustained a fall whilst hiking. An otherwise fit and active woman, this was an isolated closed injury with minimal to know soft tissue injury, and unremarkable NV examination. Initial swelling was significant, delaying definitive operative management pending improvement of local soft tissue conditions. In addition to a standard preoperative CT, the patient also received an MRI, which demonstrated intact ligamental structures, but a complete peripheral lateral meniscocapsular dissociation. both anterior an posterior roots were intact.
Preoperative Plan
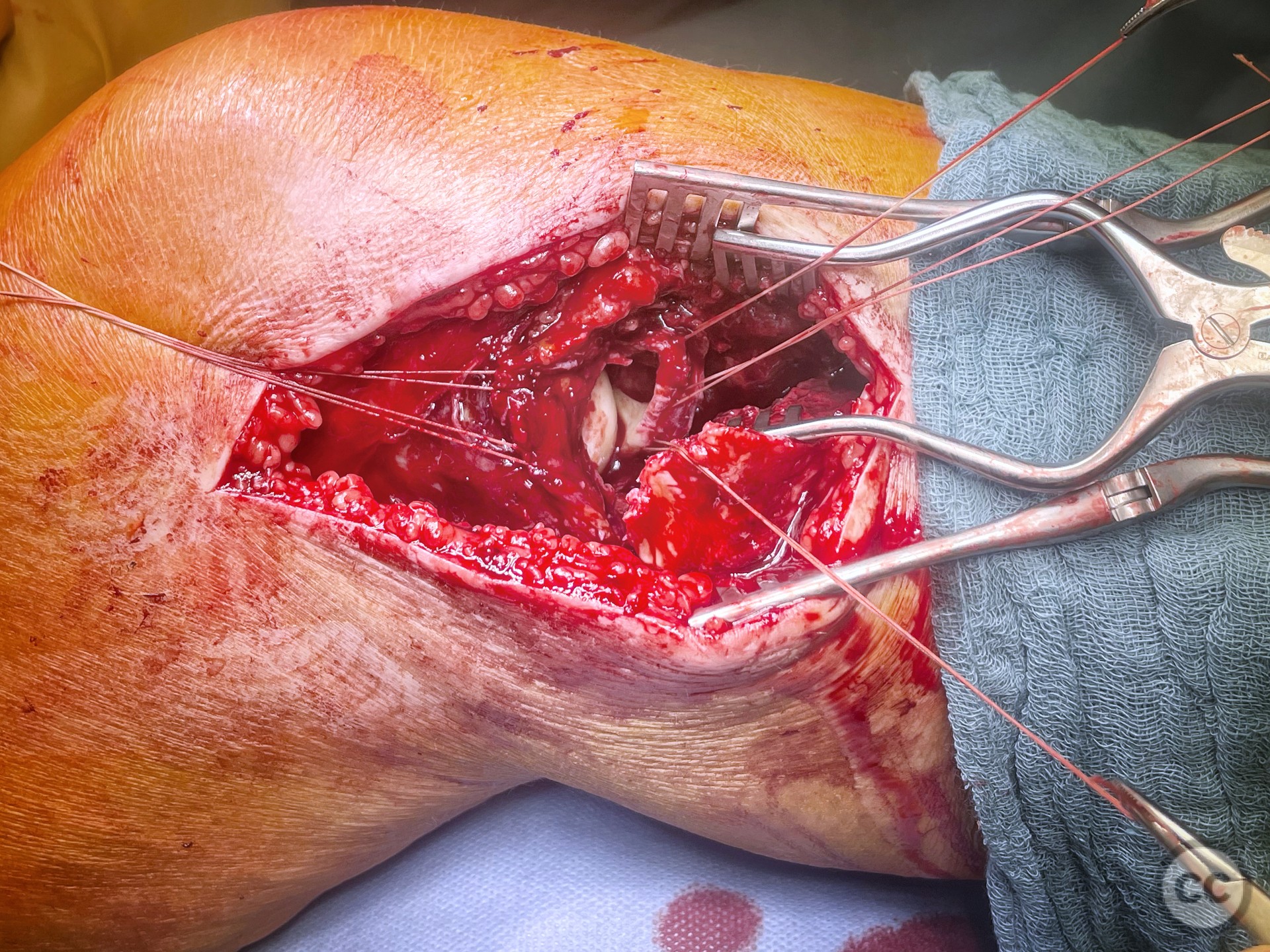
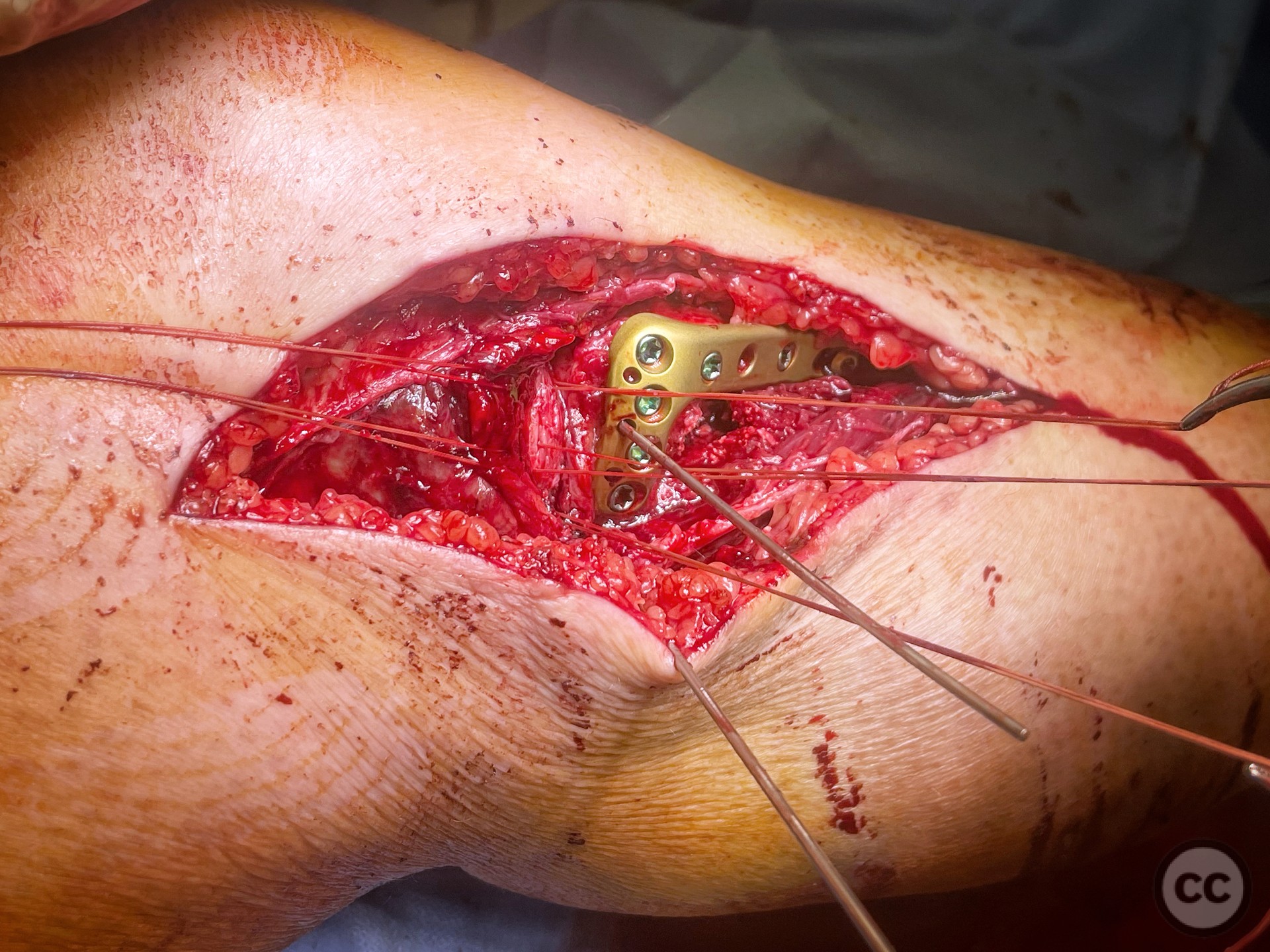
Planning remarks: Planned approach is a classical anterolateral incision, with the intention to open book the lateral split fragment, and directly address the articular depression. Sequential reassembly of the plateau from central to peripheral, utilising inside-out wires, before "closing the door" and applying a lateral plate. Depending on fragment constellation, fragment specific screw rafting, or plate bound screw rafting would be considered to support the reconstructed surface. no additional medial approach was planned.
Surgical Discussion
Patient positioning: Supine, with a carbon roll placed under the thigh allowing resting intraop flexion of 20-30deg
Anatomical surgical approach: Longitudinal anterolateral approach, splitting ITB with subperiosteal elevation from Gerdy's
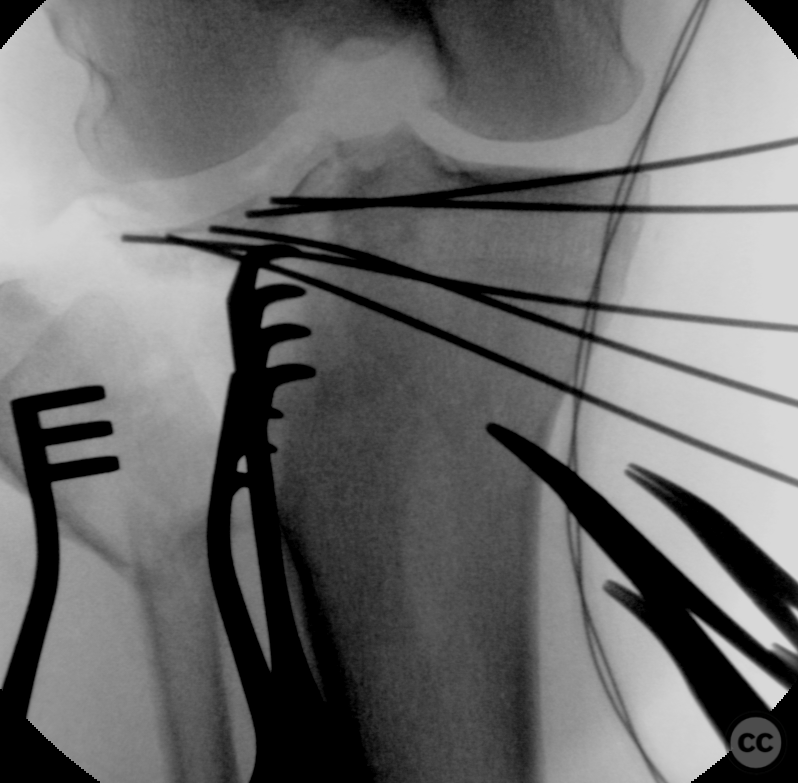
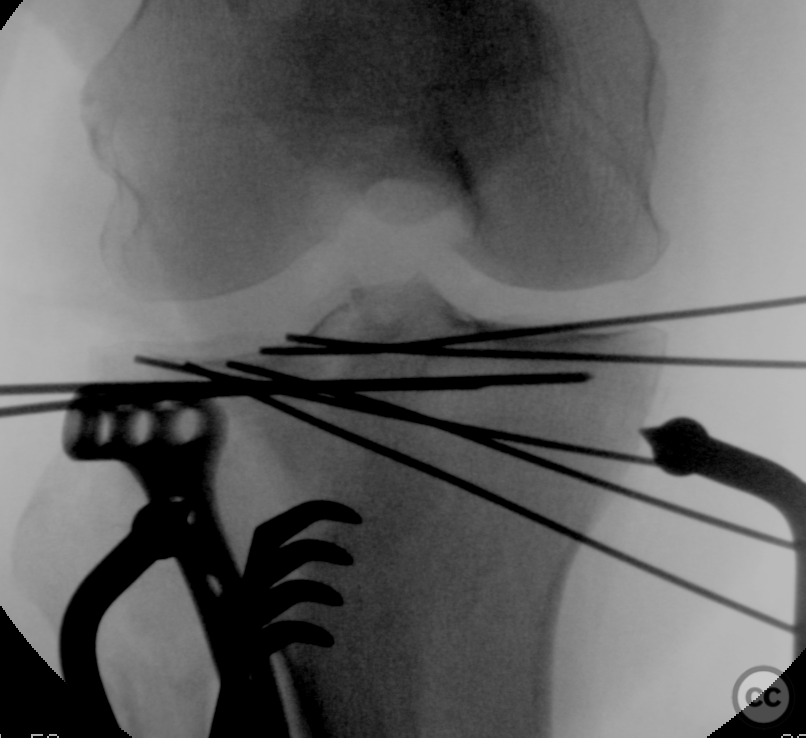
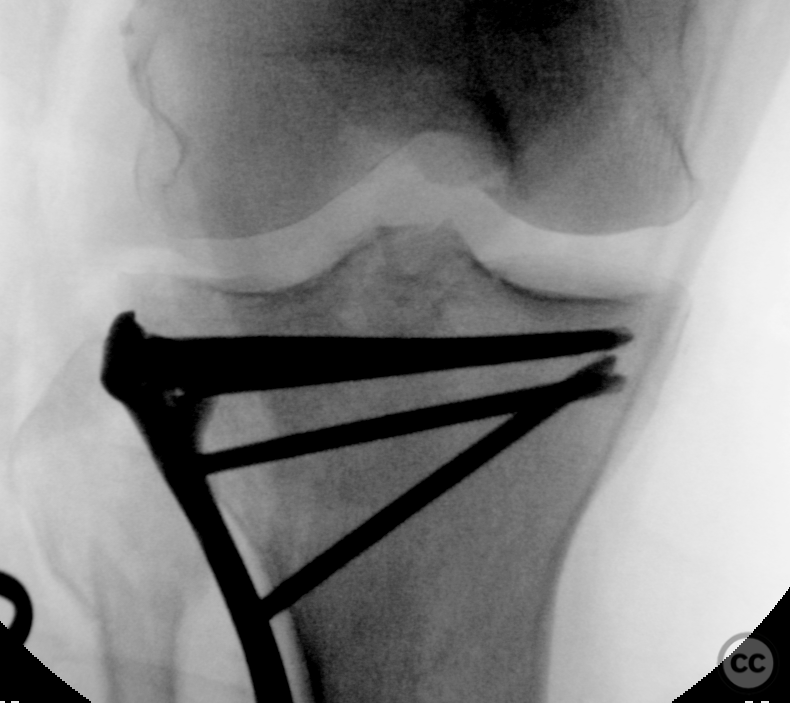
Operative remarks:Intraoperative course followed the preoperative plan. There were a significant number of independent depressed fragments extending into the lateral aspect of the eminentia. These required individual reconstruction, sequentially resulting in a large number of inside-out wires supporting the various stages of reconstruction. I had little faith that these stacked pieces would remain in place on removal of the wires - so augmented the temporary wire fixation with PLLA wire subchondral rafting spanning multiple pieces. This PLLA raft construct was then supported by graft and locked screw rafting once the 'door was closed' with reduction of the lateral splat fragment.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 960 times
14 Feb 2023
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2023). Schatzker II split depression with complete meniscocapsular separation. Journal of Orthopaedic Surgery and Traumatology. Case Report 33134530 Published Online Feb 14 2023.