








Complex Trimalleolar Ankle Fracture with Medial Soft Tissue Compromise
Score and Comment on this Case
Clinical Details
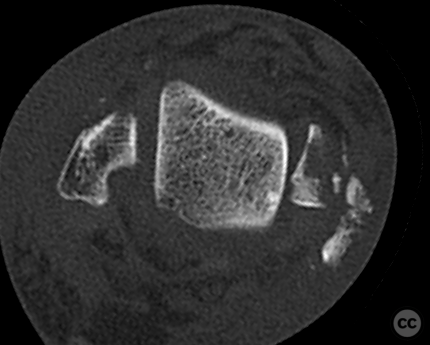
Clinical and radiological findings: A 45-year-old female patient presented to the emergency department following a trip and fall while recreational walking, resulting in a fracture dislocation of the right ankle. Initial management by paramedics included reduction and immobilization with a vacuum splint. Radiological assessment post-application of an external fixator revealed a trimalleolar fracture pattern. The fracture constellation included a Mason and Molly type 2A posterior malleolus fracture, a grossly multifragmentary medial malleolus fracture with anterior collicular and multiple posterior avulsion fragments, and a transsyndesmotic multifragmentary lateral malleolus fibular fracture. Significant soft tissue swelling and an area of threatened skin necrosis over the medial malleolus were noted.
Preoperative Plan
Planning remarks: The preoperative plan involved addressing the complex medial malleolus fracture through a combined medial and modified posteromedial approach, utilizing intraoperative 3D Cone Beam imaging for guided reconstruction. The lateral malleolus was to be stabilized using a combination of posterior anti-glide and lateral plating techniques. Syndesmotic stabilization was planned due to full-thickness AITFL rupture. and 2A fracture combination
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table with the affected limb wedged under ipsi and contralteral hemipelvis to allow for access to both posteromedial and lateral aspects of the ankle from a supine position.
Anatomical surgical approach: A medial approach was utilized to expose the medial malleolus, allowing for direct visualization and management of the multifragmentary fracture. A modified posteromedial window was created for reduction and fixation of the posterior malleolus using a mini fragment plate. The lateral malleolus was approached laterally, with additional exposure posteriorly for anti-glide plate placement.
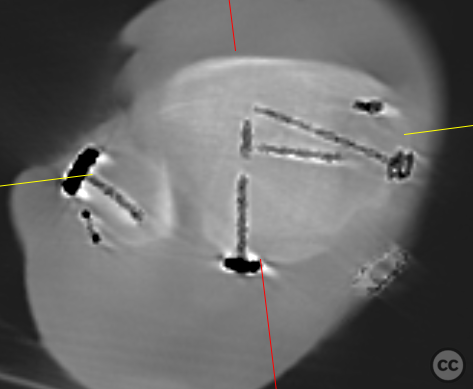
Operative remarks:Intraoperative findings confirmed the complexity of the medial malleolus fracture, with multiple avulsion fragments complicating reduction efforts. Intraoperative 3D Cone Beam imaging facilitated radiologically guided reconstruction of the medial joint mortise. Fragment-specific fixation was achieved using a 2.0 mm mini fragment plate and locking screws, supplemented by transosseous sutures for posterior avulsions and a suture anchor for the anterior collicular fragment. The lateral malleolus required dual plating due to unexpected multifragmentary nature, with a 2.4 mm posterior anti-glide plate and a 2.7 mm lateral plate employed to stabilize the fracture. Syndesmotic stabilization was achieved with two tricortical screws.
Postoperative protocol: Postoperatively, the patient was placed in a non-weight-bearing status for six weeks, with gradual progression to partial weight-bearing as tolerated. Range of motion exercises were initiated early to prevent stiffness, with emphasis on maintaining joint mobility.
Follow up: Not specified.
Orthopaedic implants used: 2.0 mm mini fragment plate, 2.4 mm posterior anti-glide plate, 2.7 mm lateral plate, suture anchor, transosseous sutures, two tricortical syndesmotic screws.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
User Discussion (1)
Juan Varela
Great reduction Size of the medial plate?
tiny thing - 2.0mm minifrag. collicular fragment was midget sized
Congratulations...well done!