





Capitellar shear fracture with concomitant radial head
Score and Comment on this Case
Clinical Details
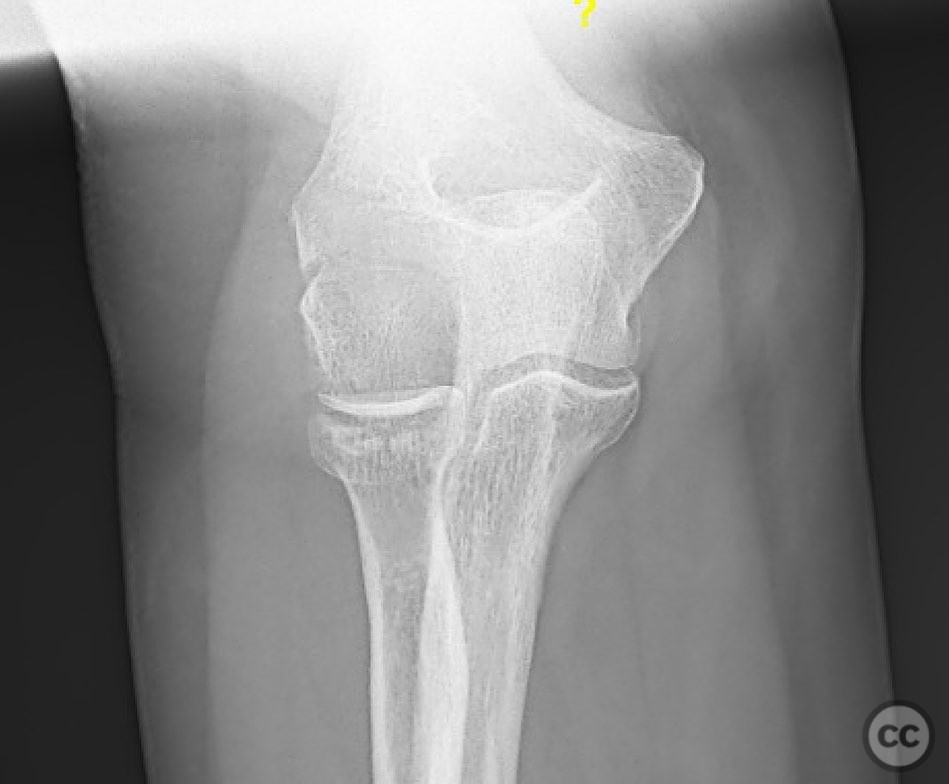
Clinical and radiological findings: 61yo fell. Presents with elbow pain and swelling. This is a capitellum (and a little bit of trochlea) shear fracture + radial head. This is a very recognizable fracture, but relatively uncommon. Before we talk surgery let’s talk ED management. These are absolutely closed reducible fractures. Extension, varus, pressure on the fragment followed by flexion and viola (maybe). It’s worth a try.
Preoperative Plan
Planning remarks:
Surgical Discussion
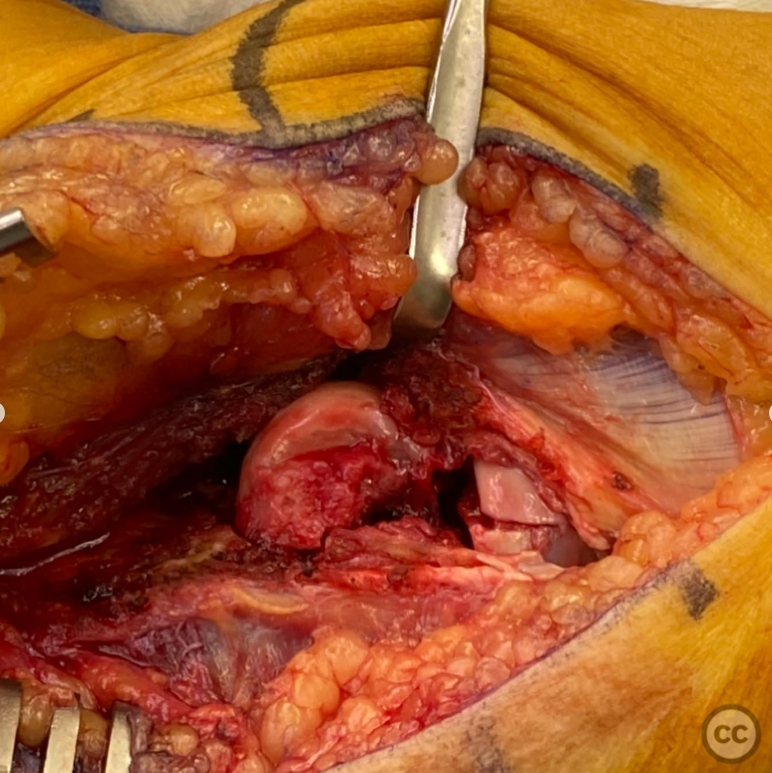
Operative remarks:Major disclaimer here- I don’t do arthroscopic surgery. For those who do and are skilled at elbow scoping, please discuss the tips and tricks. If open reducing, exposure is key. The fracture is simple, but visualization and implant location/trajectory can be tricky. Kocher approach. The LUCL is rarely injured in this pattern so the elbow is stable. As such, 2) you need to surgically destabilize the elbow to reduce the fracture and get screws perpendicular to the fracture. You can do this either by doing a lateral epicondyle osteotomy or by taking the common extensor origin and anterior capsule off as a sleeve while leaving the LUCL intact. This was a smaller patient so I decided to sleeve off the common extensor origin. Fixation is anterior to posterior countersunk 2.0 lag screws and a back up orthogonal screws. The radial head was repairable (1.5 and 1.3mm screws). If it wasn’t- excision of the fragments is a option but ranging the elbow after excision is KEY! There’s a high likelihood of a catch point between the caudal capitellum exit (where there is a little comminution) and the radial head excision step. If that’s the case, the radial head should be replaced. If not, the radial head will pop the capitellum off. Lastly, repair common extensor origin with a double loaded suture anchor! Post-op- splint for a week, then transition to a thermoplastic removable splint.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1218 times
15 Jan 2023
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2023). Capitellar shear fracture with concomitant radial head. Journal of Orthopaedic Surgery and Traumatology. Case Report 34351807 Published Online Jan 15 2023.