









Distal 1/3 humerus shaft fracture - a lateral paratricipital approach with proximal split window
Score and Comment on this Case
Clinical Details
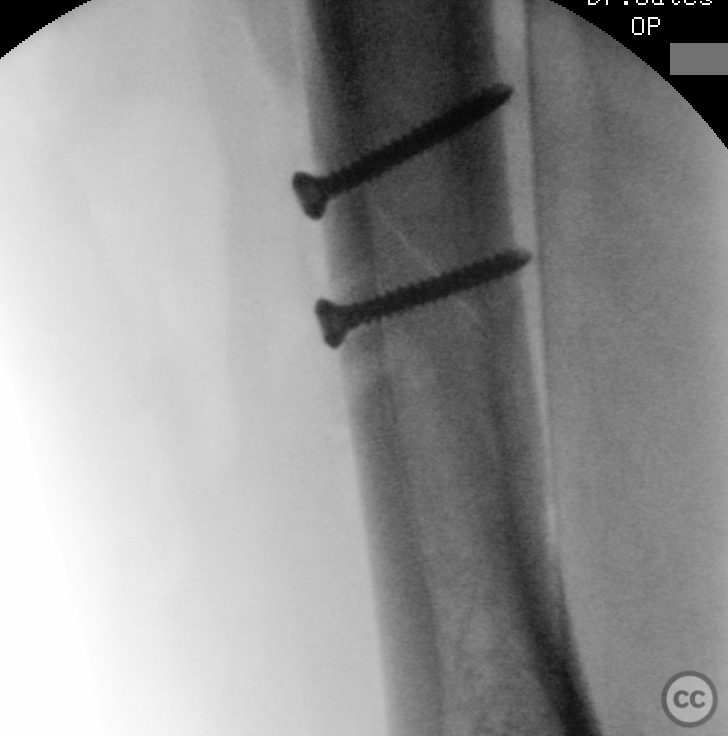
Clinical and radiological findings: This case is one of a 25 year old female who fell from a horse at a moderate speed. She sustained a closed distal 1/3 diaphyseal fracture of the humerus, with no primary neurological symptoms. The patient presented initially to a regional hospital where imaging and splint immobilisation were performed. The patient was subsequently referred to our clinic and following discussion, it was clear she sought a rapid recovery without the use of an orthosis, and consented and proceeded with an open reduction and dorsoradial locking plate fixation.
Preoperative Plan
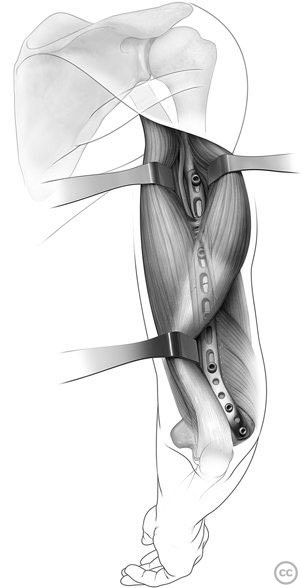
Planning remarks: The classical surgical approach for a dorsoradial plate is the elevation of a long paratricipital window along the radial border of the lateral head of triceps, elevating triceps from the intermuscular septum to the level of the deltoid. Rather than mobilise the entire triceps posteriorly, I prefer to limit mobilisation to the level of the perforation of the radial nerve through the septum. This working window is often sufficient for visualisation and reduction of the majority of distal 1/3 fractures without having to do a complete radial neurolysis. Proximal plate fixation can then be done in a minimally invasive muscle splitting fashion between the medial and lateral heads of triceps in the middle to proximal third of the humeral shaft offering convenient drill access and axis. Here the course of the radial nerve and its associated peripheral nerve bundles are easily identified and mobilised with minimal risk of neuropraxia. Despite dramatic intraoperative photos, these patients complain of remarkably little post operative pain and benefit from early mobilisation.
Surgical Discussion
Patient positioning: Prone
Anatomical surgical approach: Lateral paratriciptal
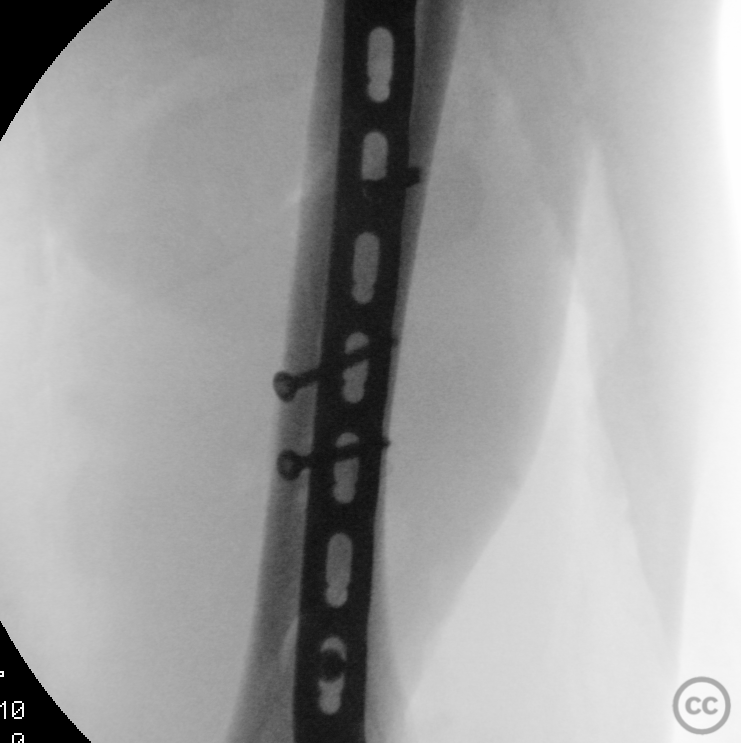
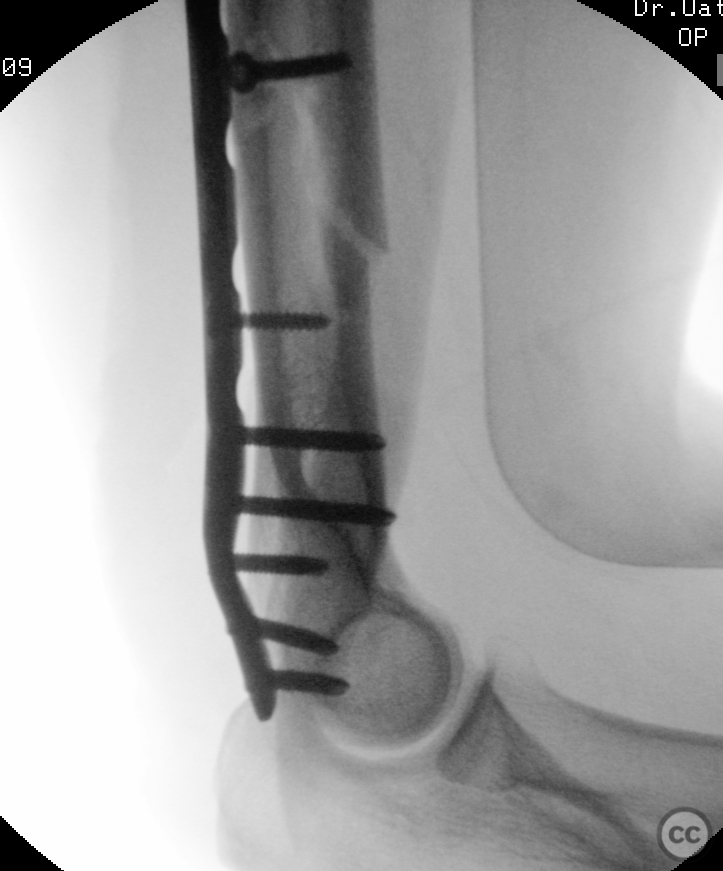
Operative remarks:Operation was performed prone with the arm resting on a small side support table, the forearm flexed 90deg towards the floor. Midline posterior approach to the humerus, elevation of a lateral paratricipital window from the lateral intermuscular septum - utilising the ascending course of the posterior antebrachial cutaneous nerve as a guide to find the perforation of the radial nerve through the septum. The fracture was reducible entirely through the lateral window distal to the radial nerve. A small medial paratricipital window anterior to the ulnar nerve was opened for lag screwing before positioning the plate. To facilitate proximal plate fixation without having to mobilise the lateral belly of triceps (and with it the radial nerve) we opened an additional proximal working window between long and lateral heads of triceps. Proximal to the aponeurosis it is a simple matter to identify and mobilise the descending course of the radial nerve bundle, protect it, and proceed with proximal instrumentation and plate fixation. One of my favourite operative approaches - the anatomy is always a treat. My favourite quiz for residents whist dissecting the radial paratricipital window is the course of the posterior cutaneous antebrachial nerve. This can be considered a lighthouse for the radial nerve and courses along the distal aspect of the intermuscular septum and is easily identifiable, embedded in or on the septum. Whilst elevating triceps and following the nerve proximally, staying in the plane of the nerve will lead you directly to the radial nerve as it emerges through the septum. This is a reliable landmark and key to safe and quick preparation of this surgical window. The relationship of the radial nerve as it passes through the radial groove on the posterior aspect of the humerus is identifiable through the landmark of the apex aponeurosis on the dorsal aspects of the triceps fascia. The course of the radial nerve can be predicted as being two finger breadths proximal to the apex of the aponeurosis. Alternatively, it can be measured as 2.5 centimetres or one inch. Both the surgical approaches and the use of the aponeurosis landmark and the posterior cutaneous antebrachial nerve are referenced in the reading material below.
Orthopaedic implants used: DePuy Synthes 3.5mm posterolateral extraarticular humerus plate.
PubMed® Literature Review
Generated by The Literature - Realtime PubMed® AnalysisThe lateral paratricipital approach is a surgical technique used for the treatment of humerus fractures and involves accessing the fracture site through a lateral incision and mobilizing the radial nerve as necessary [1]. An anatomical study by Gerwin et al. (1996) investigated the course of the radial nerve in relation to operative exposures of the posterior aspect of the humeral diaphysis [2]. They found that the radial nerve crossed the posterior aspect of the humerus, with several branches innervating the lateral head of triceps but none innervating the medial head. Based on their findings, they developed three operative approaches: posterior triceps-splitting, proximal radial nerve mobilization, and modified posterior approach [2]. In a retrospective study by Eglseder (2012), supracondylar distal humeral fractures treated with fracture-specific plating and a lateral approach with medial triceps mobilization technique were reviewed [4]. The study aimed to evaluate preoperative and postoperative radial nerve palsies (RNP) and determine if there was an impact on RNP rates based on plating and fixation techniques. The incidence rate of known preoperative RNP was high in both blunt injury group (27%) and gunshot wound group (20%). However, postoperative RNP rates were similar to those reported in literature despite using a lateral approach with medial triceps mobilization technique [4]. A randomized controlled study by Teng et al. (2023) compared combined medial and lateral approach versus paratricipital approach in open reduction and internal fixation for type C distal humerus fracture [6]. The study included 37 patients with type C distal humerus fracture who underwent open reduction and internal fixation. The combined medial and lateral approach group had a longer sum of incision length compared to the paratricipital approach group, but there was no significant difference in operation time, blood loss, or Caja score. At 3 months postoperatively, the combined approach group had higher Mayo Elbow Performance Score (MEPS), but there was no significant difference at 6 months postoperatively or at the last follow-up [6]. In a retrospective case-control study by Gibbs et al. (2022), the rate of postoperative radial nerve palsy (RNP) in humeral shaft nonunion reconstruction was investigated [9]. They found that none of the cases treated with a lateral paratricipital approach developed postoperative RNP, while cases treated with triceps splitting approach had a significantly higher rate of new RNP. The study suggests that the lateral paratricipital exposure decreases the risk of radial nerve injury during nonunion reconstruction of the humerus [9].
Conclusion:
The lateral paratricipital approach is a viable surgical technique for treating humerus fractures. It provides adequate exposure while minimizing damage to surrounding structures such as the radial nerve. Studies have shown that this approach can be effective in achieving anatomical reduction and restoring elbow function. However, further research is needed to compare its outcomes with other approaches and evaluate long-term results.
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 9845 times
21 Nov 2022
Add to Bookmarks
DOI: 10.36438/ORIF2022001 Full Citation
Full Citation
Cite this article:
Oates, E.J. (2022). Distal 1/3 humerus shaft fracture - a lateral paratricipital approach with proximal split window. Journal of Orthopaedic Surgery and Traumatology. Case Report 34614029 Published Online Nov 21 2022. DOI: 10.36438/ORIF2022001