



















Subluxed Moore 2 / Schatzker IV tibial plateau fracture
Score and Comment on this Case
Clinical Details
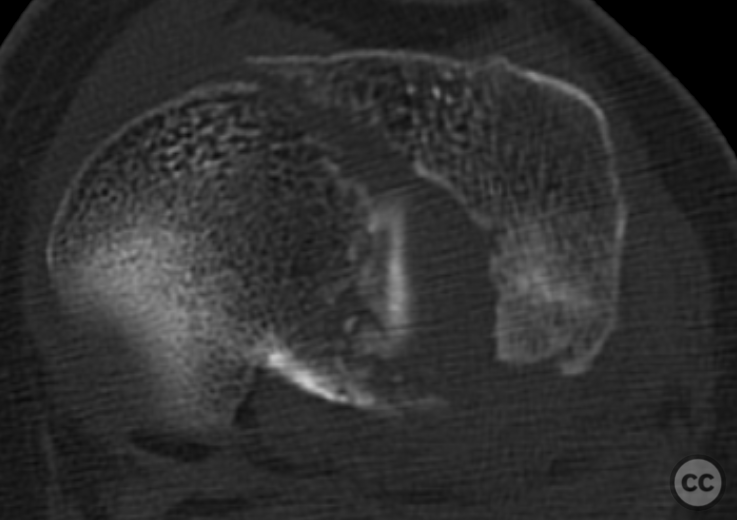
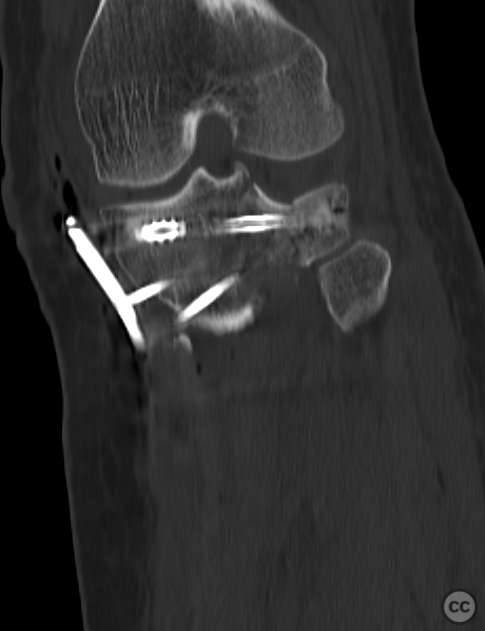
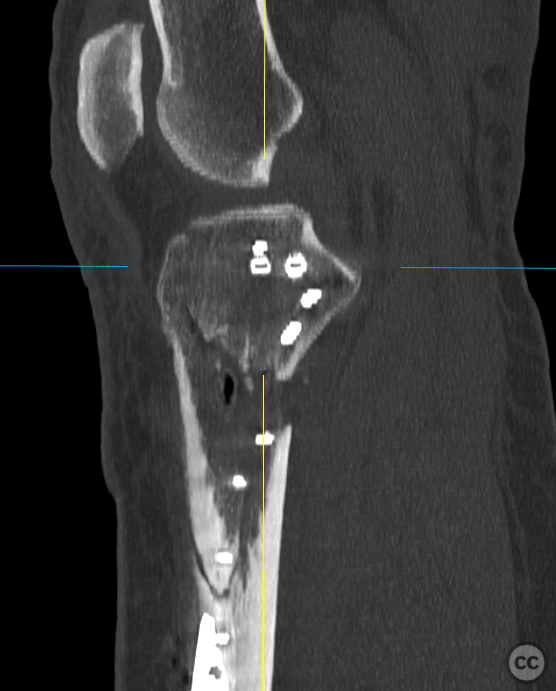
Clinical and radiological findings: A 67-year-old female presented after a domestic fall, unable to weight bear on her left leg. Clinical examination revealed a closed injury with significant swelling, deformity, and intact neurovascular status. Plain radiographs and CT imaging demonstrated a comminuted Moore 2 / Schatzker Type IV tibial plateau fracture with an intact lateral cortex, depressed but intact lateral aspect of the lateral condyle, and significant articular depression of the medial aspect of the lateral condyle extending into the eminentia. The eminence and medial tibial condyle were fractured and medially displaced, resulting in subluxation of the knee joint. The medial articular surface was spared from direct fracture involvement.
Preoperative Plan
Planning remarks: The preoperative plan aimed to preserve the intact lateral cortical column and reconstruct the medial column, restoring joint axis and bicondylar height. The central lateral joint depression presented a challenge due to its inaccessibility from the intact lateral side and the block-split nature of the medial condylar injury.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table with a carbon roll under the proximal thigh to allow 30 degrees of knee flexion and 270-degree circumferential access to the tibial plateau.
Anatomical surgical approach: A dual-window approach was utilized with longitudinal incisions over the medial and lateral aspects of the knee. The medial approach was larger due to distal fracture extension, while a limited lateral approach involved an osteotomy window at the inferior aspect of Gerdy's tubercle for indirect reduction of the central lateral articular surface using a bony tamp.
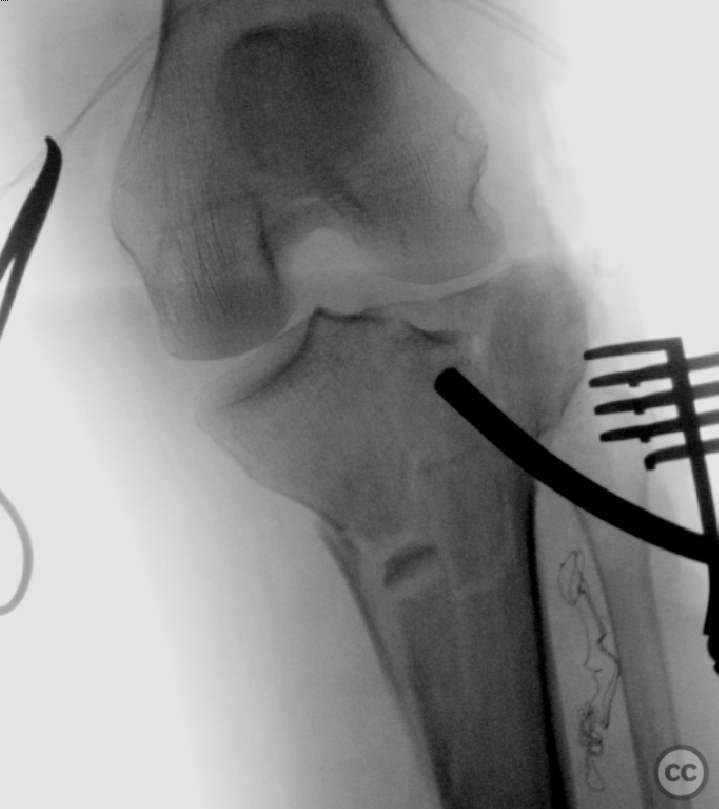
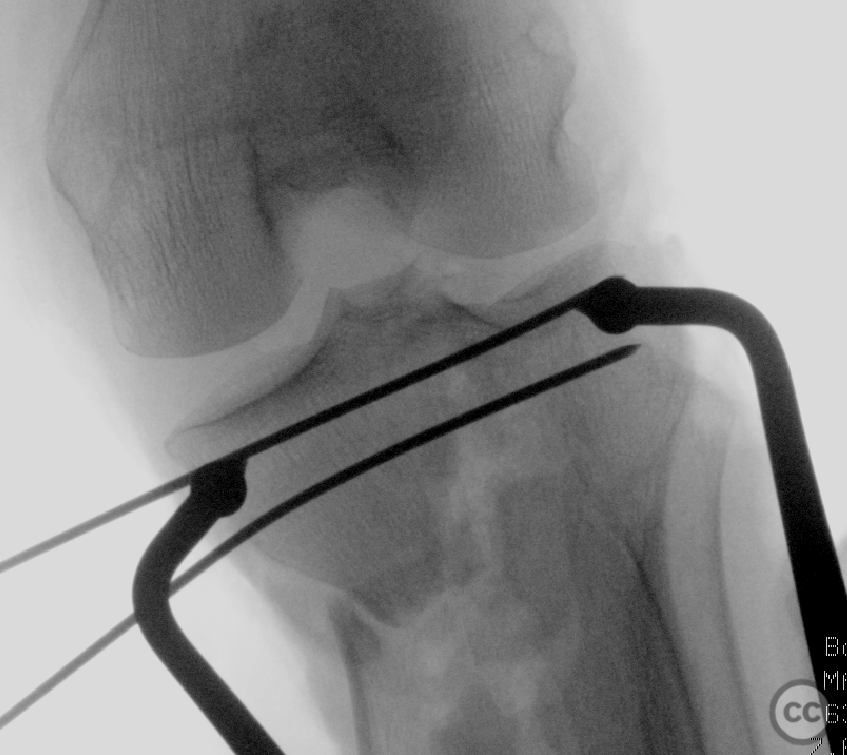
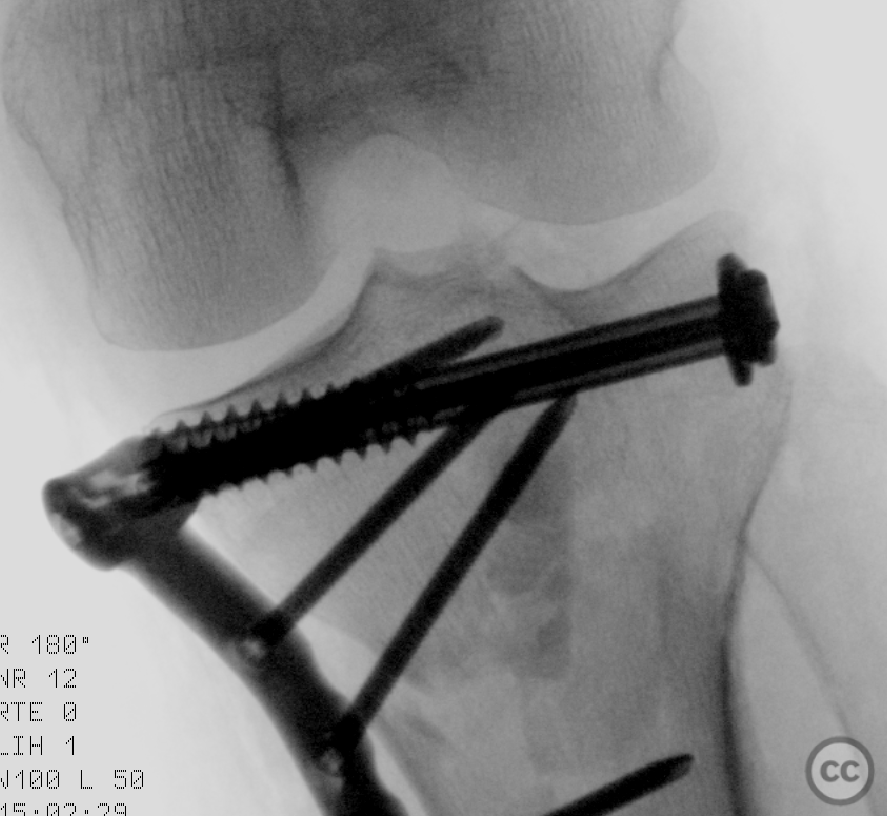
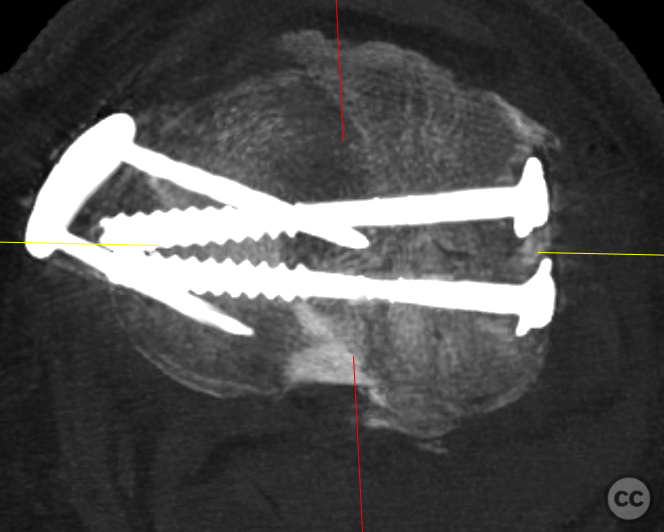
Operative remarks:Intraoperatively, indirect reduction of the central lateral articular surface was challenging but achieved by elevating the depressed fragment to its approximate articular height through lateral window osteotomy and medial intrafocal manipultaion before being provisionally secured to the medial block with K-wires. This reduced articular surface and medial condylar block were then reduced en bloc to the intact lateral column. The restored, now intermediate, lateral articular fragment did lose some reduction during this en block manouver. Medial column height was restored by reducing the large intermediate fragment at the metaphyseal-diaphyseal transition, which included the superficial medial collateral ligament insertion, restoring valgus stability. A large bone reduction clamp compressed the femoral condyles before introducing two 6.5mm cannulated rafting screws laterally to medially, engaging the medial block fragment. An anteriomedial 3.5mm buttress plate with locking rafting screws was used to support the medial column and to secure medial collateral integrity.
Postoperative protocol: Postoperatively, the patient was managed in a knee orthosis to reduce valgus stress, with immediate encouragement of free range of motion. Non-weight bearing was maintained for eight weeks, progressing to full weight bearing by ten weeks.
Follow up: At 18 months follow-up, the patient demonstrated a pain-free range of motion from 0 to 140+ degrees, with a slight valgus axis compared to the contralateral side and no clinically identifiable ligamentous instability. No impedement of activity reported.
Orthopaedic implants used: Two 6.5mm cannulated screws (lateral to medial) - Anterior medial 3.5mm buttress plate with locking rafting screws
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
User Discussion (1)
Salar Ahmed
Would be an added bonus if patient positioning, surgical incisions/markings and implant pictures were added too. Very satisfying to see the great outcome
Sure, I can try to get more comprehensive images on future cases. I dont necessarily plan cases which i upload, most are done retrospectively