









Displaced Greater Tuberosity Fracture with Associated Bankart Lesion.
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 49-year-old male presented following an electrical shock injury, with a resultant left shoulder injury. Initial radiographic evaluation revealed a displaced fracture of the greater tuberosity (troquiter). A subsequent computed tomography scan confirmed significant displacement of the greater tuberosity and identified a small bony Bankart lesion. Surgical intervention was indicated for the greater tuberosity fracture, while conservative management was chosen for the Bankart lesion.
Preoperative Plan
Planning remarks: The preoperative plan involved a Mackenzie approach to the shoulder, with detachment of the anterior deltoid's acromial portion to access the fracture site. The plan included traction of the fracture using sutures, provisional fixation with a Kirschner wire, and definitive fixation with transosseous high-strength sutures and partially threaded screws.
Surgical Discussion
Patient positioning: The patient was positioned in a beach chair position under general anesthesia combined with peripheral nerve block.
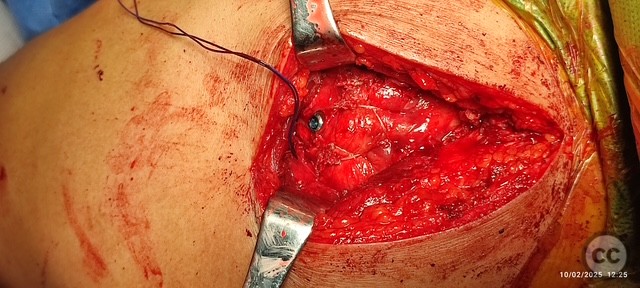
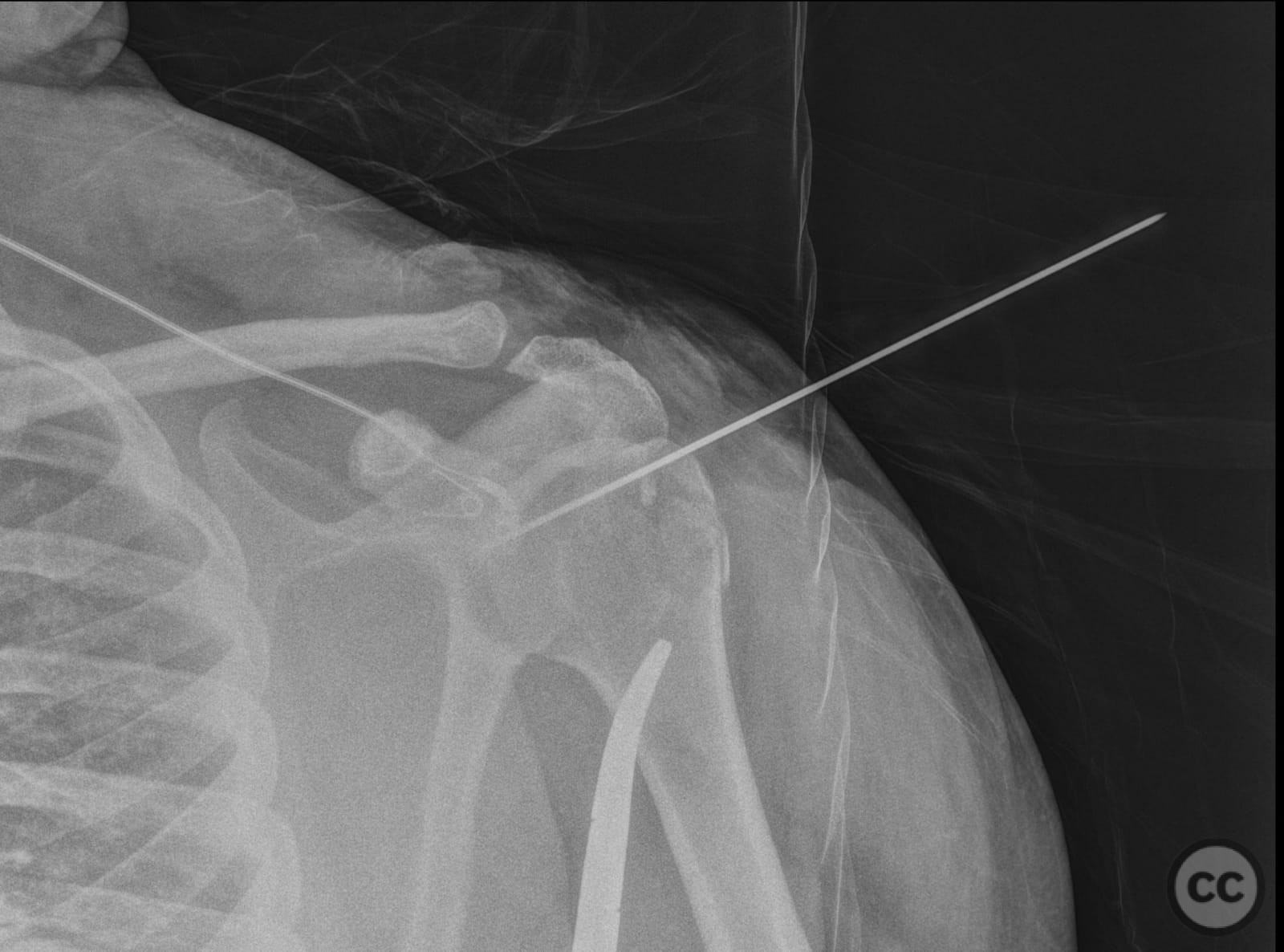
Anatomical surgical approach: A Mackenzie approach was utilized, involving an incision over the shoulder and detachment of the anterior deltoid's acromial portion. The greater tuberosity fracture was accessed, and traction was applied using sutures. Provisional fixation was achieved with a Kirschner wire. Definitive fixation involved five transosseous high-strength sutures and two 4.0 mm partially threaded screws. Reduction was confirmed intraoperatively with imaging. The deltoid was reattached using transosseous sutures, followed by skin closure.
Operative remarks:The surgeon noted that the use of high-strength sutures and screws provided stable fixation of the displaced greater tuberosity fracture. The decision to manage the associated small bony Bankart lesion conservatively was based on its size and clinical presentation.
Postoperative protocol: Postoperative rehabilitation included immobilization in a sling for initial weeks, followed by gradual passive range of motion exercises progressing to active range of motion as tolerated. Strengthening exercises were introduced in later stages of rehabilitation.
Follow up: Not specified.
Orthopaedic implants used: Kirschner wire, 5 high-strength transosseous sutures, two 4.0 mm partially threaded screws.
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
User Discussion (1)
Dr Ed Oates
Great job. Ive been tempted to try tape/anchor only repair, using a multistrand 'speed bridge' style fixation for these. one question - why take down deltoid, rather than logitudinal fiber-split?
thank you. Speed bridge type repair is a good alternative but very expensive for my hospital. Taking down the anterior deltoid gives you much more visibility, especially if you need to do the transosseous sutures and the reinsertion of the deltoid with transosseous sutures is quite safe to allow early rehabilitation. I stopped doing splits because I did not feel comfortable with the management of sutures because I felt like I had very little space.