






Dubberley Type IA Capitellar shear fracture
Score and Comment on this Case
Clinical Details
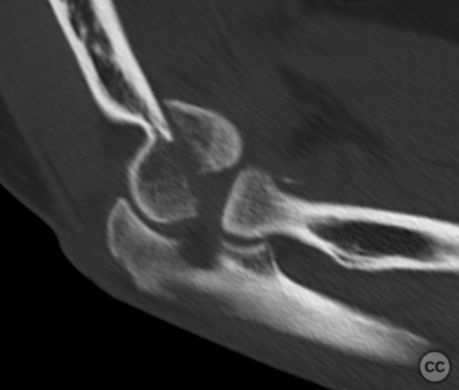
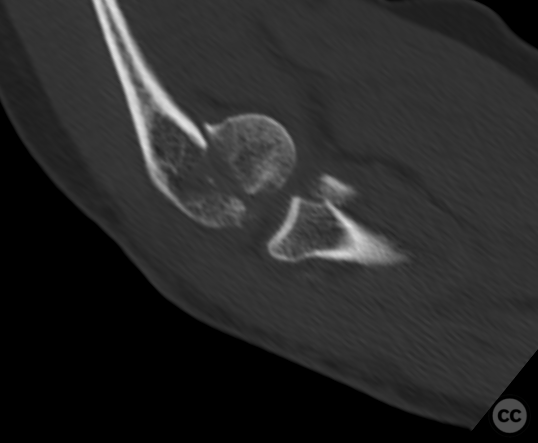
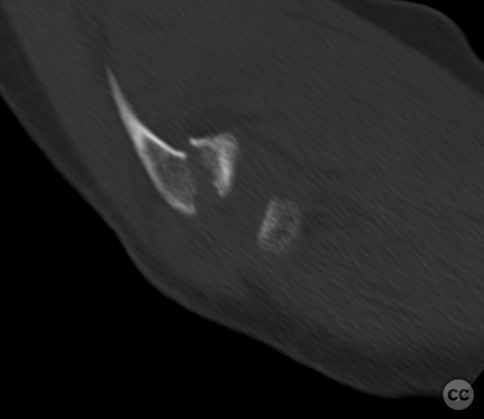
Clinical and radiological findings: This is a 45-year old man who sustained a low energy domestic full. He sustained this isolated upper extremity injury which was closed and neurovascularly intact. Plain film imaging was technically difficult and poorly executed hence not provided. The preoperative CT scans both in 3D recon and surgical reconstruction are provided. Here you can appreciate a Dubberly type 1 sub category A capital of shear injury together with a small displaced radial head fracture. The preoperative planning assumed an intact dorsal cortex, and simple screw fixation was appropriately planned.
Preoperative Plan
Planning remarks:
Surgical Discussion
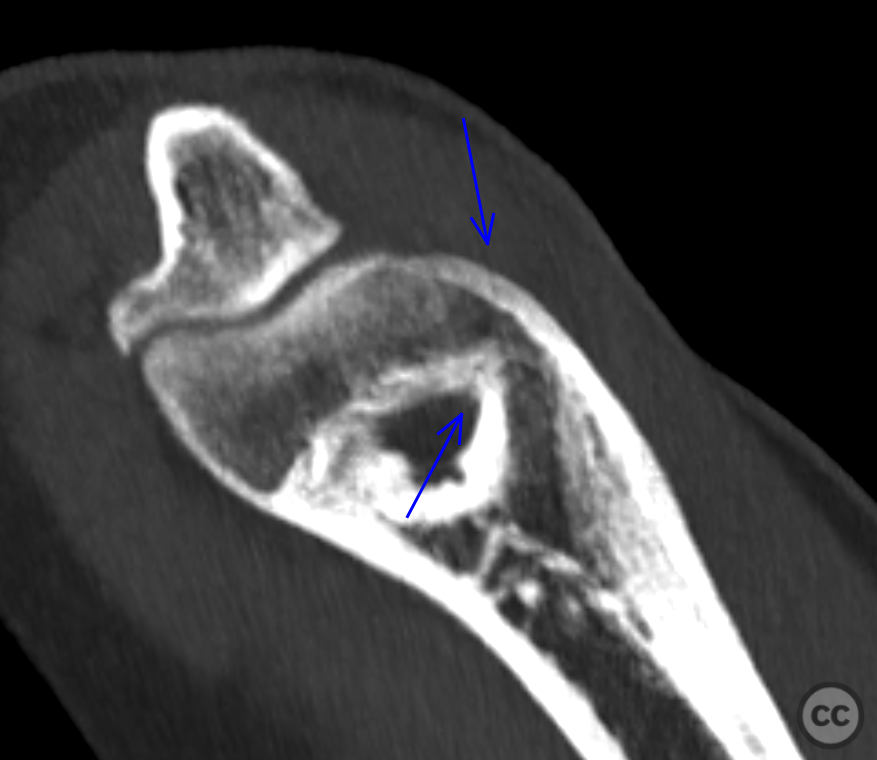
Operative remarks:Is simultaneous fixation of the radial head injury was planned, I chose a dorsal approach through Boyds interval to address both fractures. The patient was placed supine on a radio translucent operating table with the elbow flexed and the forearm placed on a board in front of the chest of the patient. Access through Boyds was unremarkable with good exposure of both fractures without needing to dissect the annular ligament or lateral ulnar collateral ligament from the supinator crest. Reduction of the capitellar fragment was initially unremarkable and for anterior-posterior headless bone screws were used to engage the anterior fragment in two planes. The radial head fracture was also easily reduced and fixed with two headless screws in a tripod technique. Unfortunately upon dynamic testing of the construct the capital fracture Torah way from the distal humerus pulling with it the the screw fixation. Retrospective forensic examination of the CT demonstrates a fine nondisplaced fracture line through the dorsal cortex. A combination of this fracture along with perforation of the cortex by multiple screw holes is likely responsible for the failure of fixation. Fortunately the dorsal voids approach allowed and easy proximal extension into the distal humerus allowing placement of a dorsoradial locking plate. This revised construct was then stable through a full range of motion allowing early rehab.
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1041 times
11 Nov 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Dubberley Type IA Capitellar shear fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 37492844 Published Online Nov 11 2022.