








Anterior-only fusion of a teardrop C6/7 fracture
Score and Comment on this Case
Clinical Details
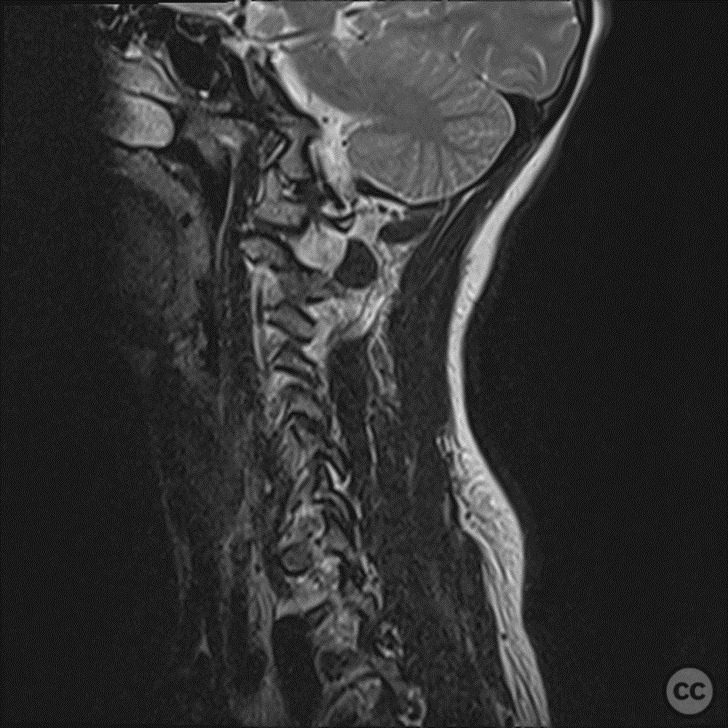
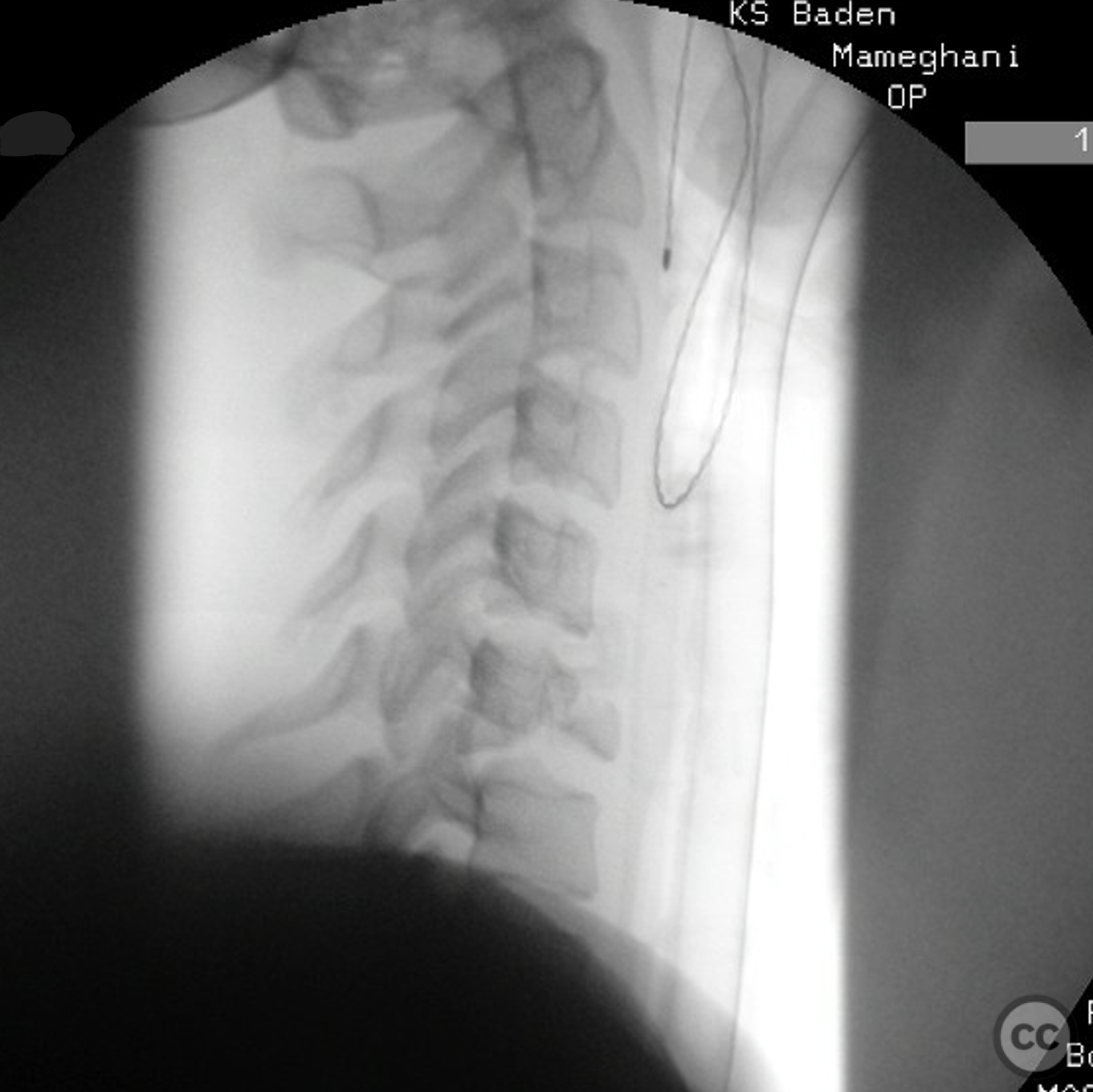
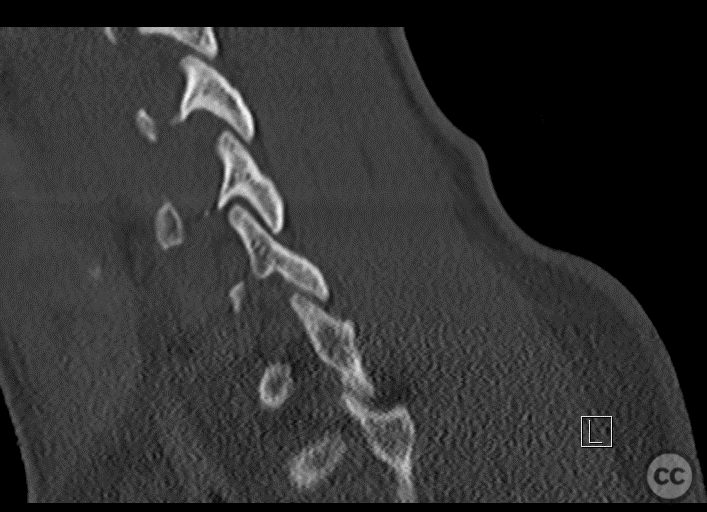
Clinical and radiological findings: 15yo girl after bicycle accident, no neurologic deficits but bilateral radicular pain (C7), walks into the ED with her father. Lateral X-ray shows typical hyperflexion/compression injury at level C6/7 with teardrop sign. CT and MRI confirm typical injury with critical spinal cord compression but without spinal cord injury. According to the AO Spine Subaxial Injury Classification System: C6/7 type B2 F4 C6:A3 N2
Preoperative Plan
Planning remarks: Anterior open reduction via Smith-Robinson approach, interposition of iliac crest C6/7 and monosegmental plating C6/7 if possible. Extension to corpectomy C6 an plating C5/7 if necessary. As the joints were displaced, but the osseous facets were intact , anterior-only approach was judged as the less invasive startegy than going anterior-posterior from the start.
Surgical Discussion
Patient positioning: supine, roll in the neck
Anatomical surgical approach: Smith-Robinson approach (from the right side, surgeon's preference)
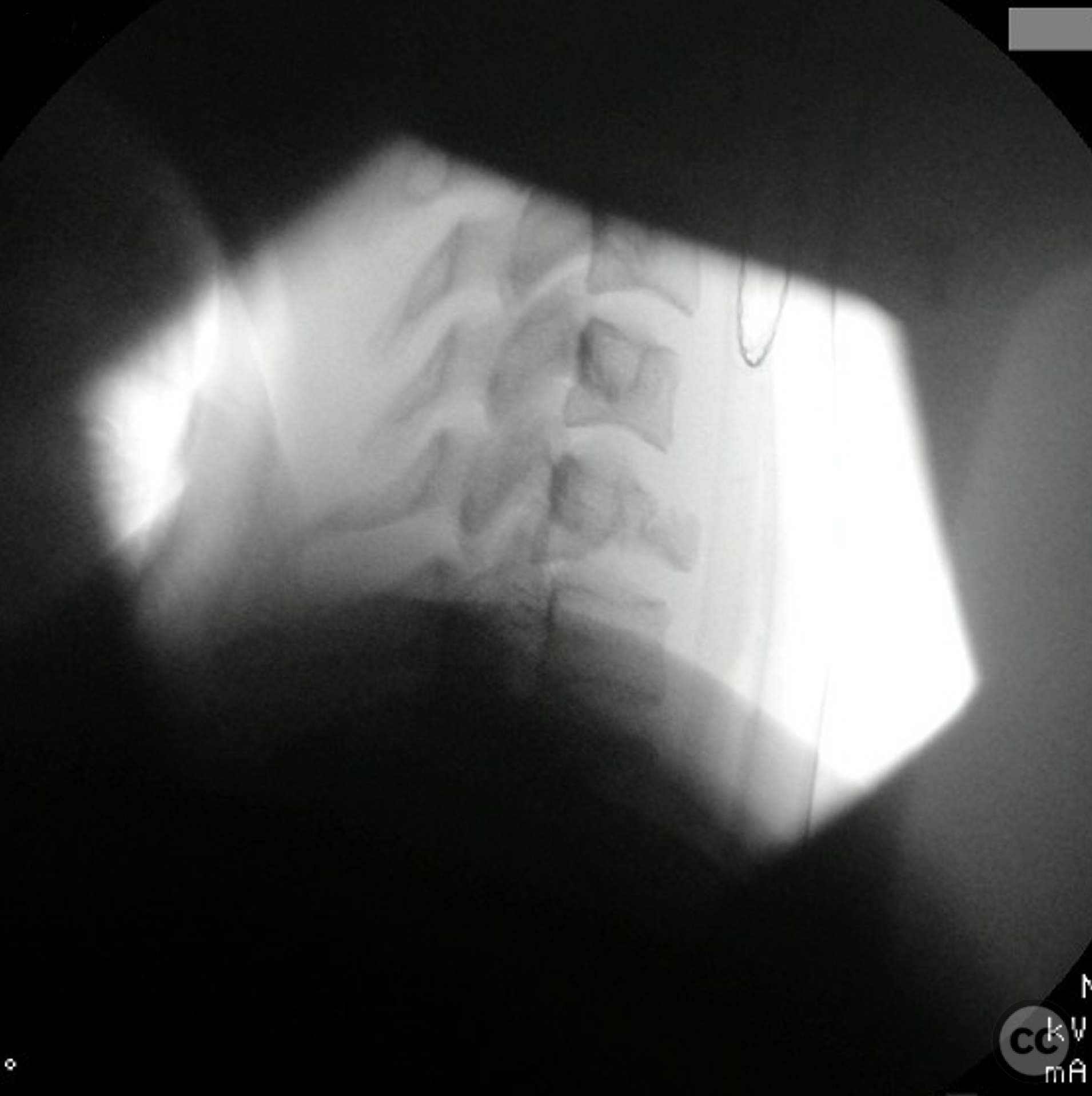
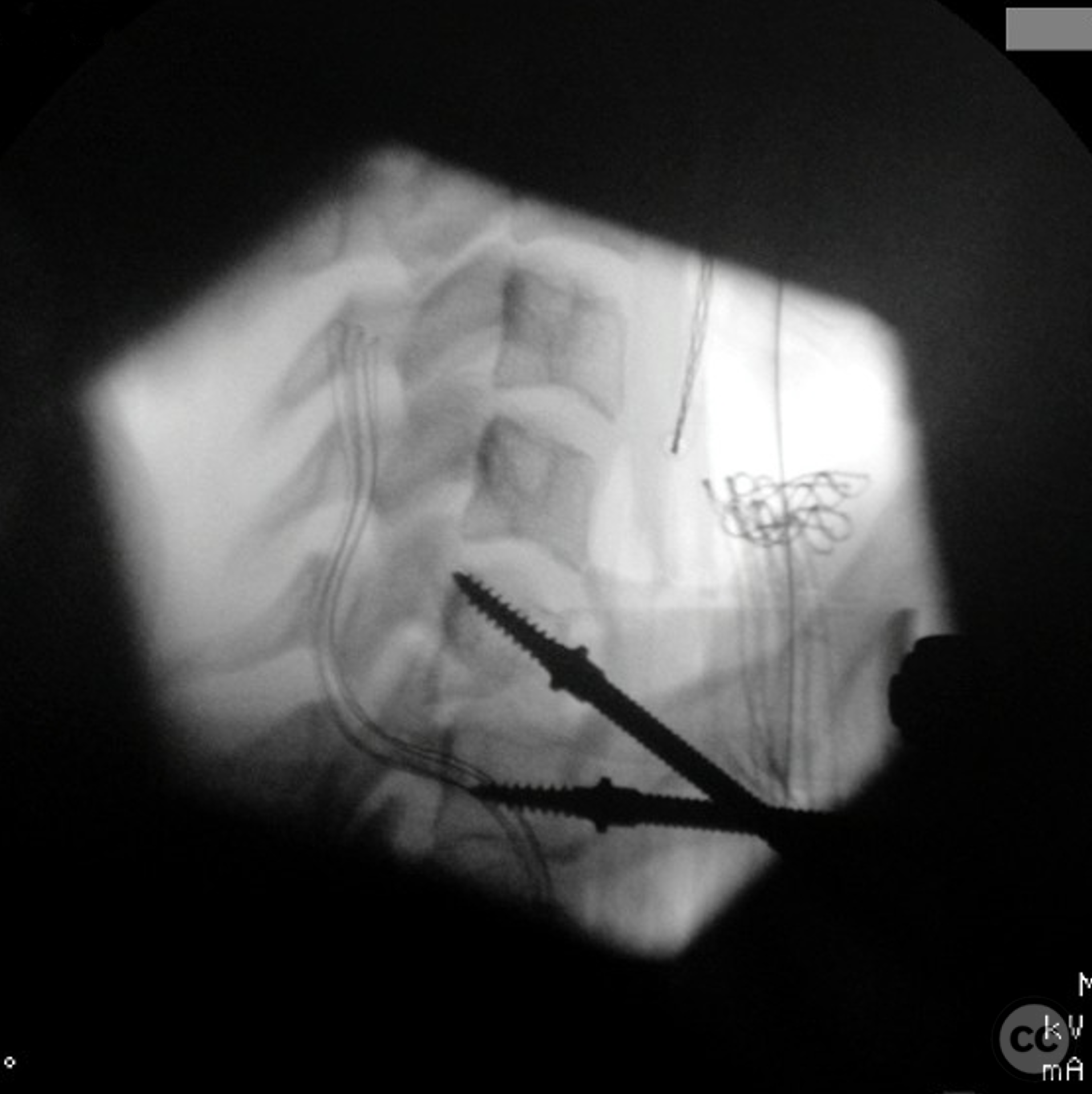
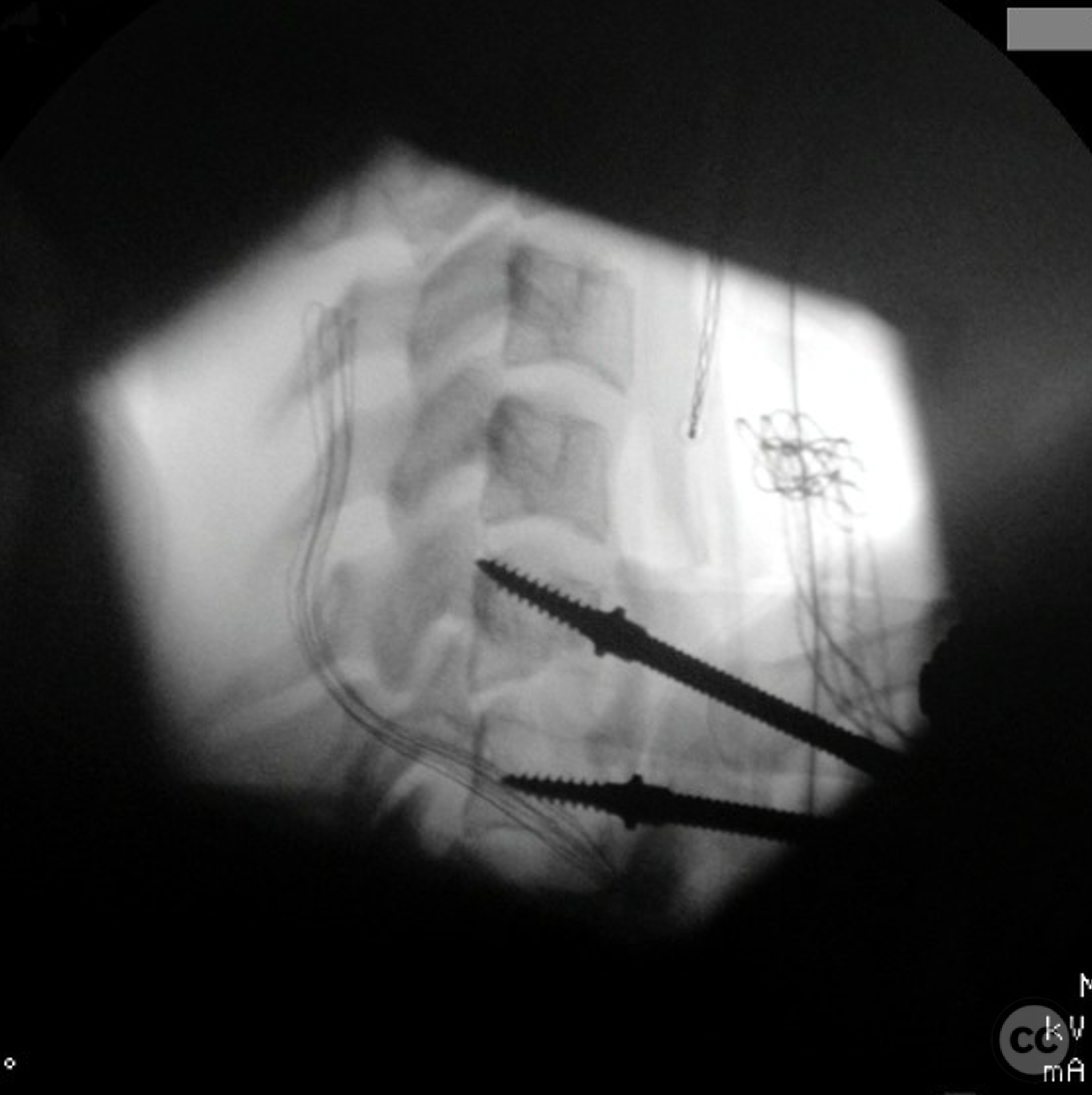
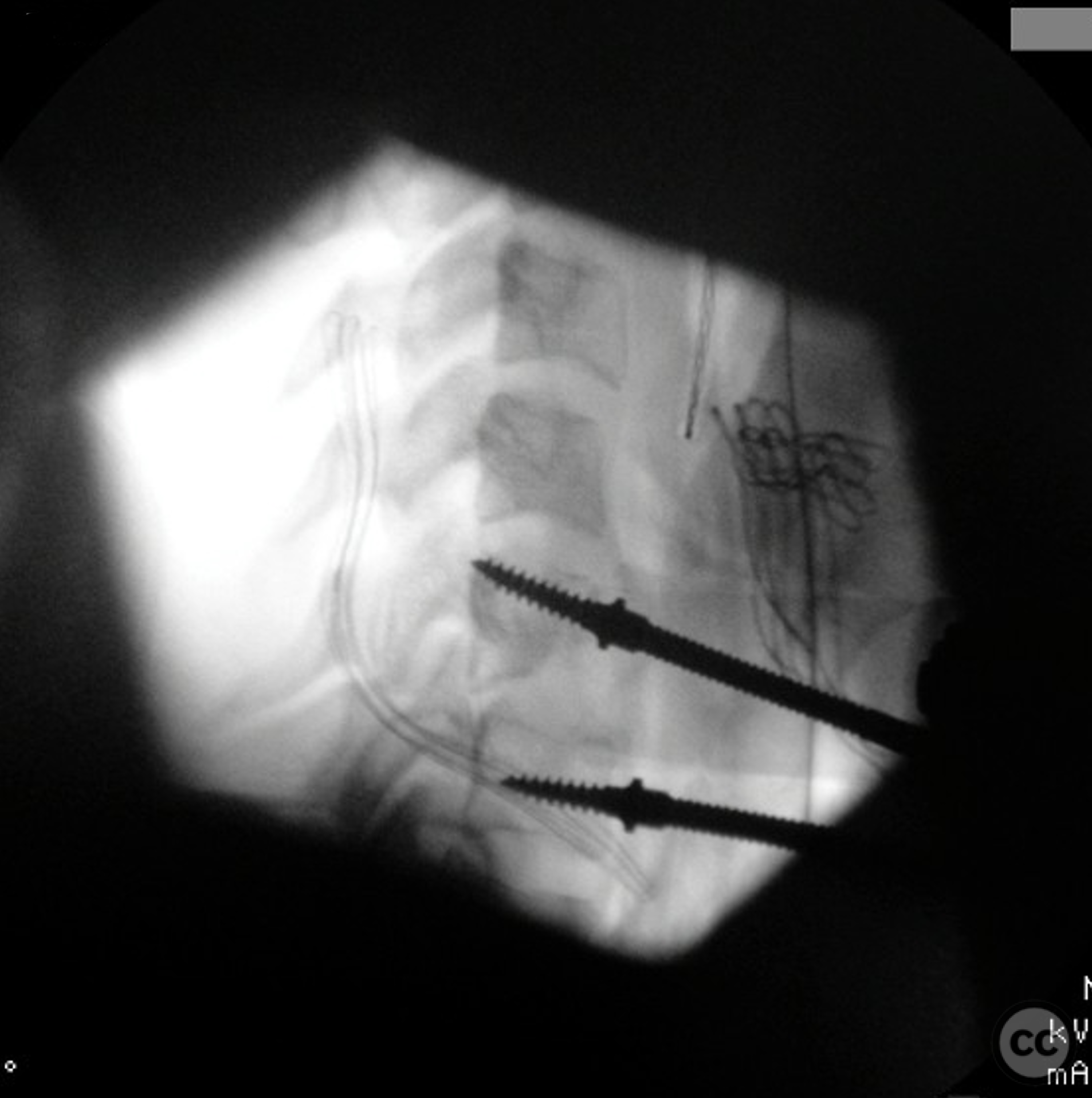
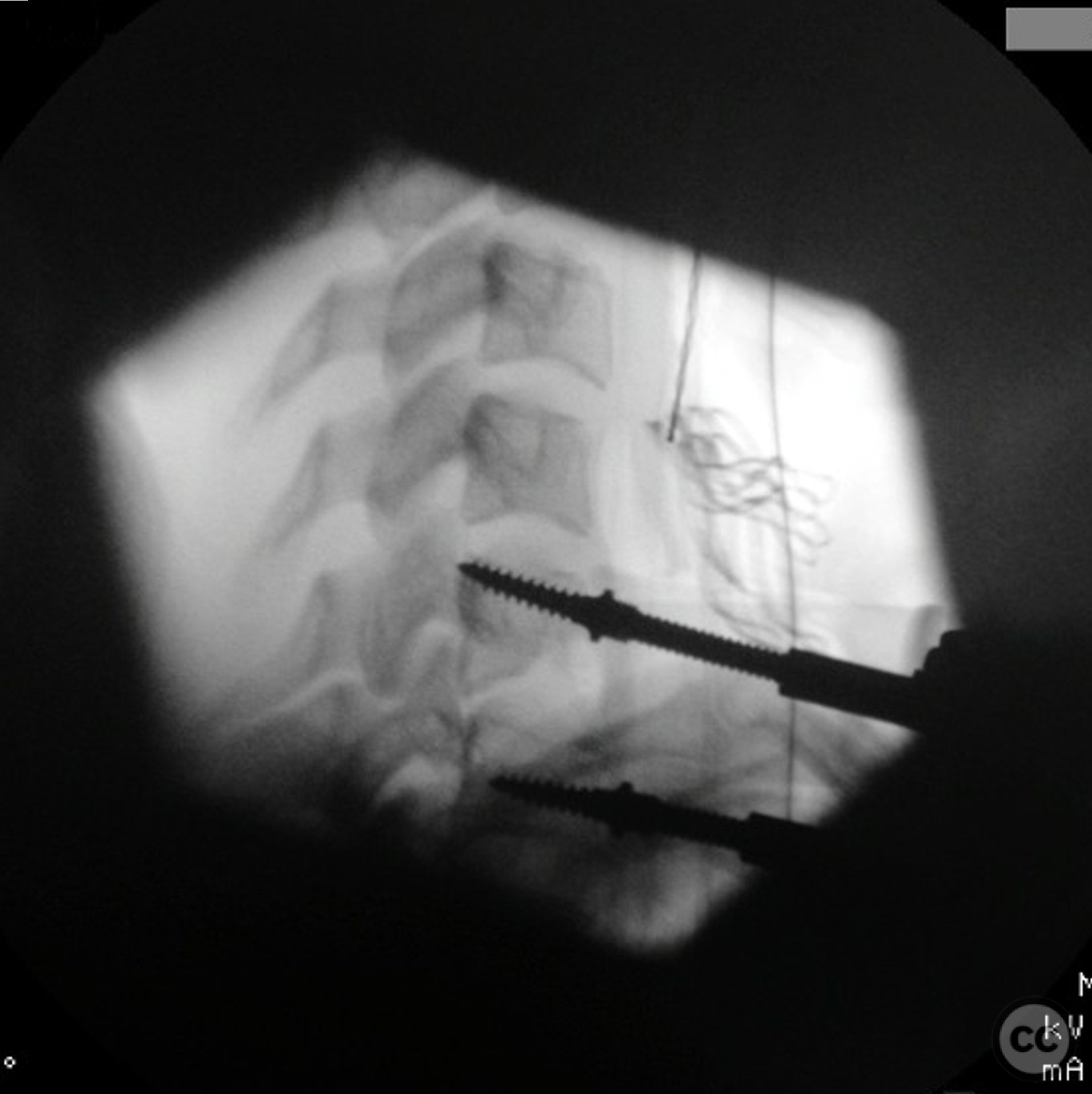
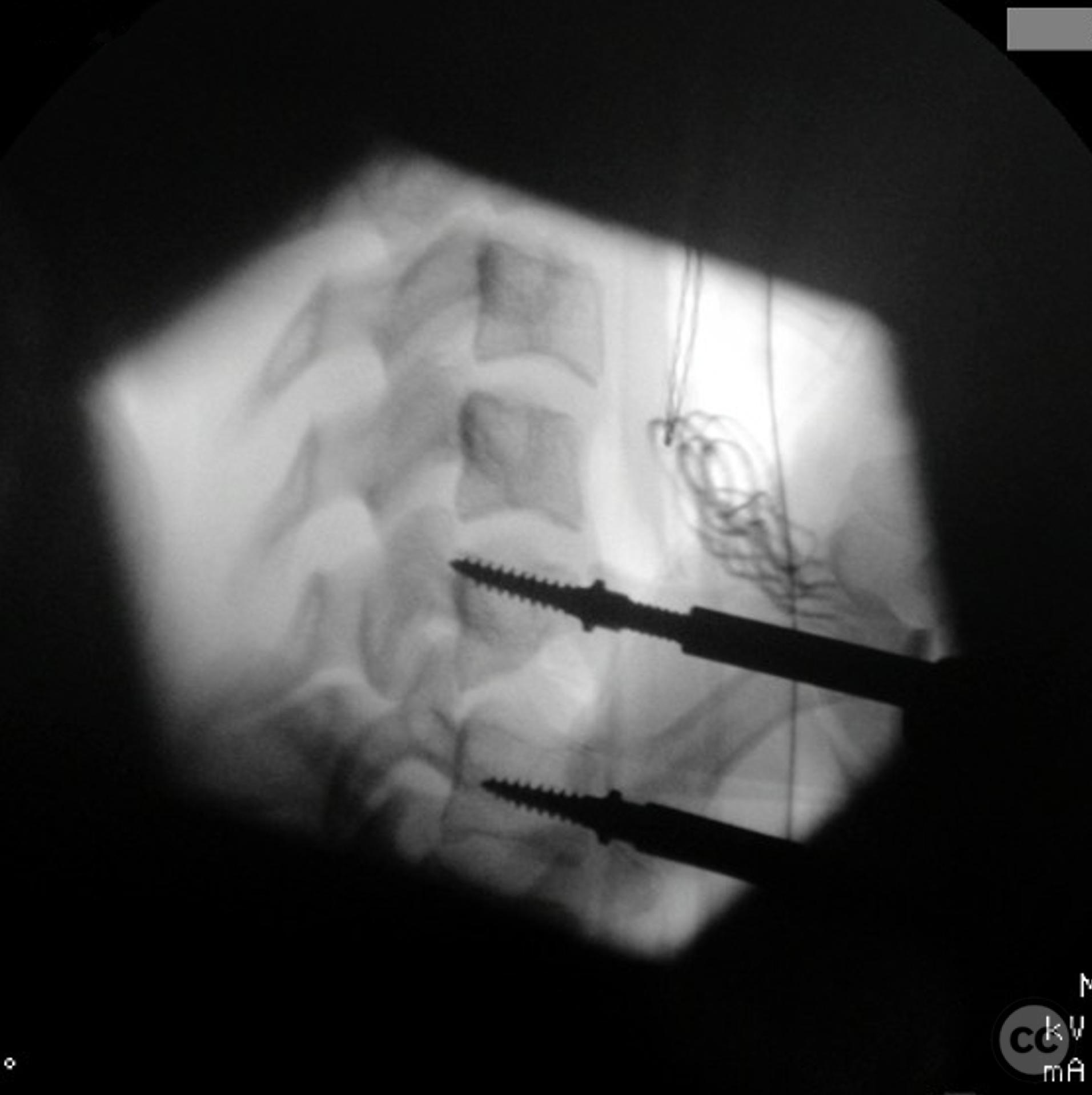
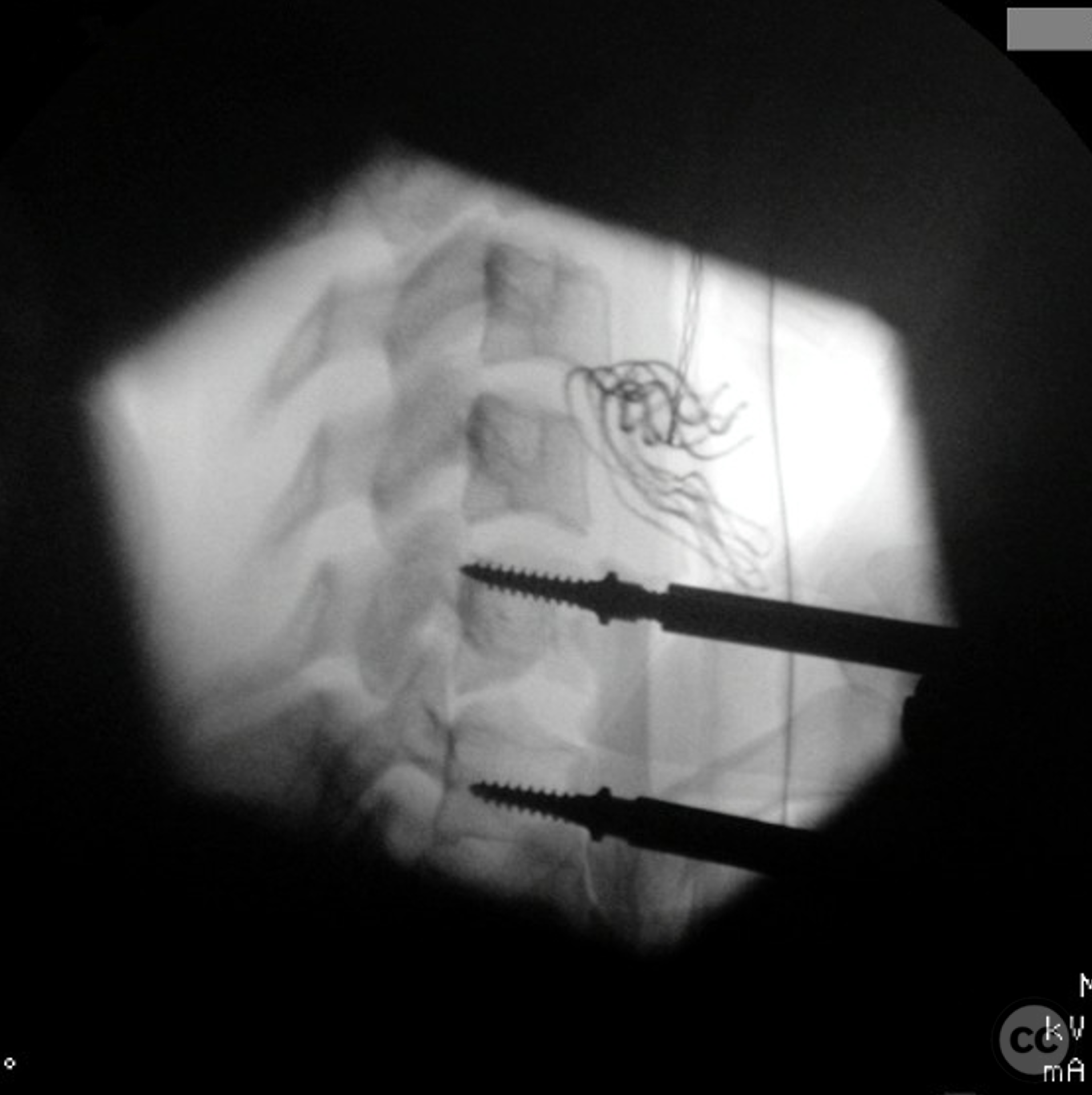
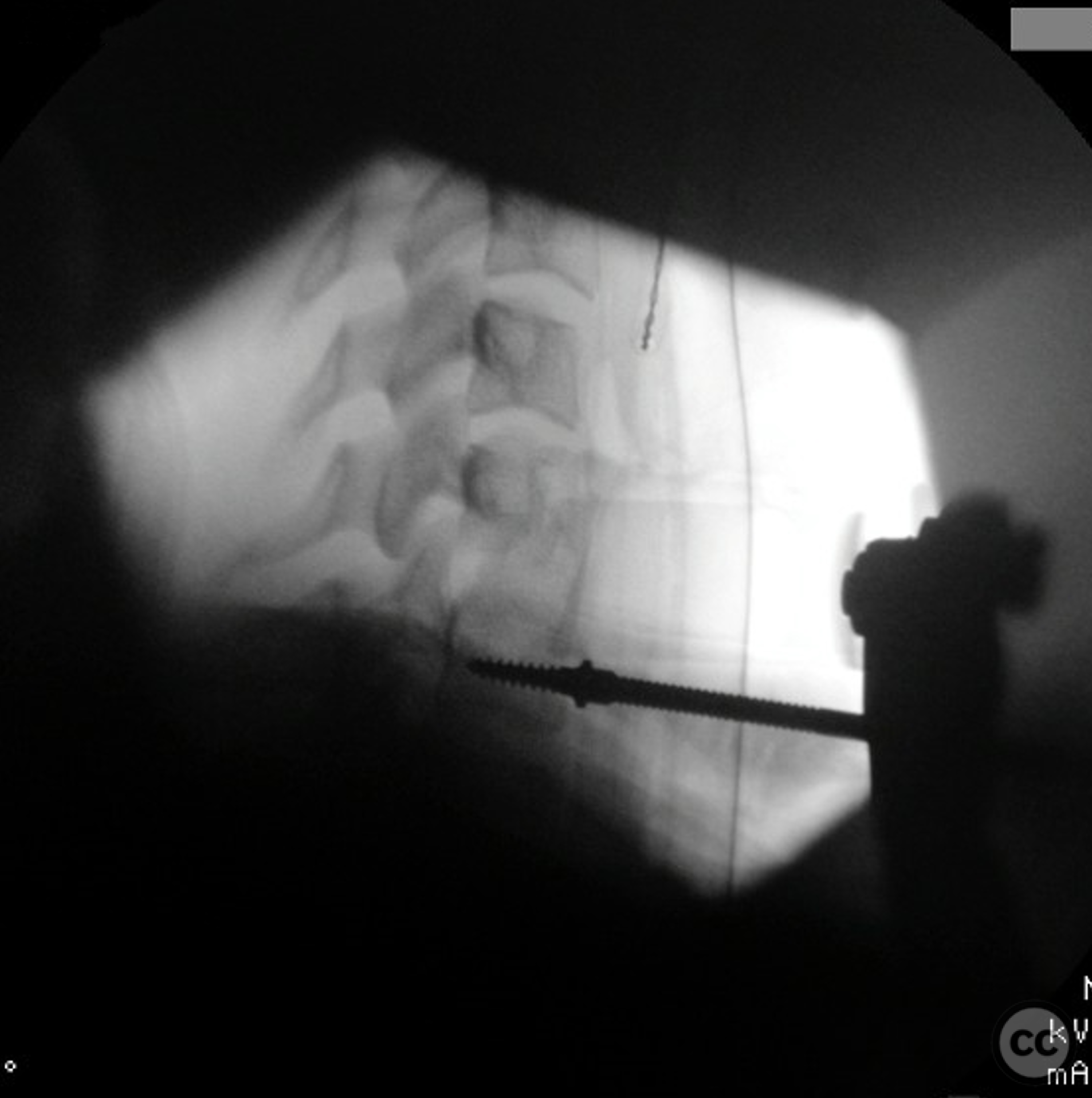
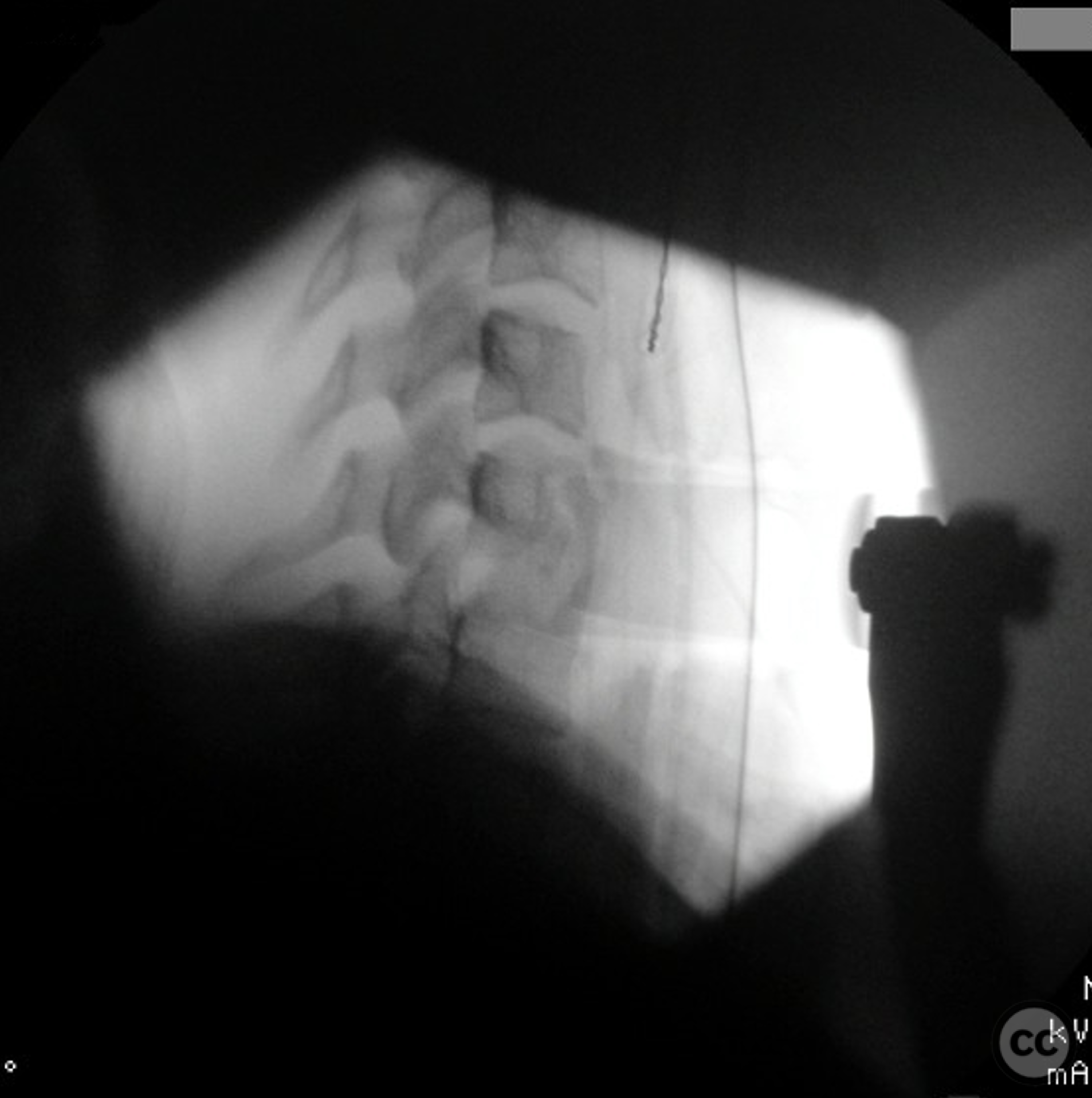
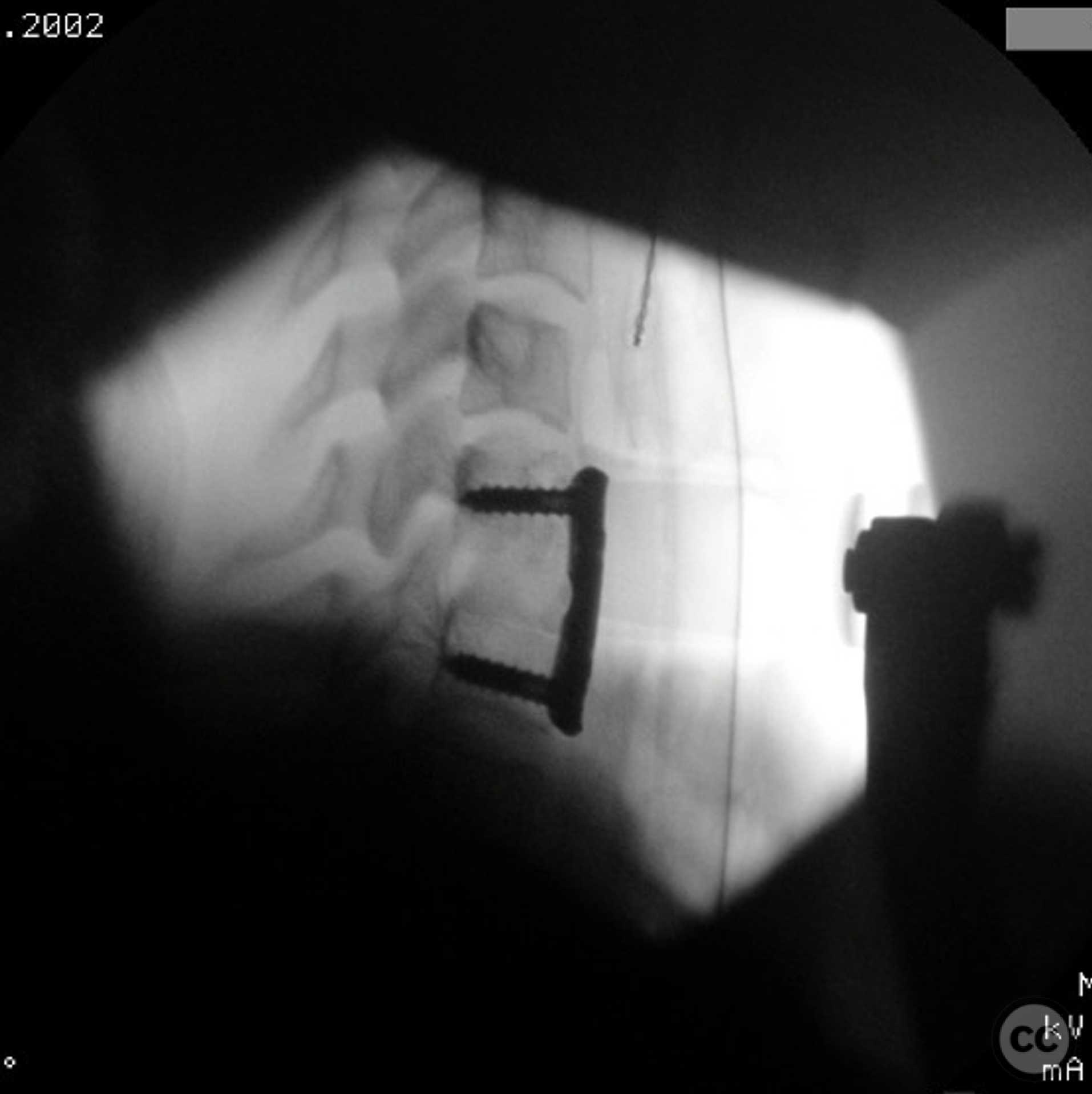
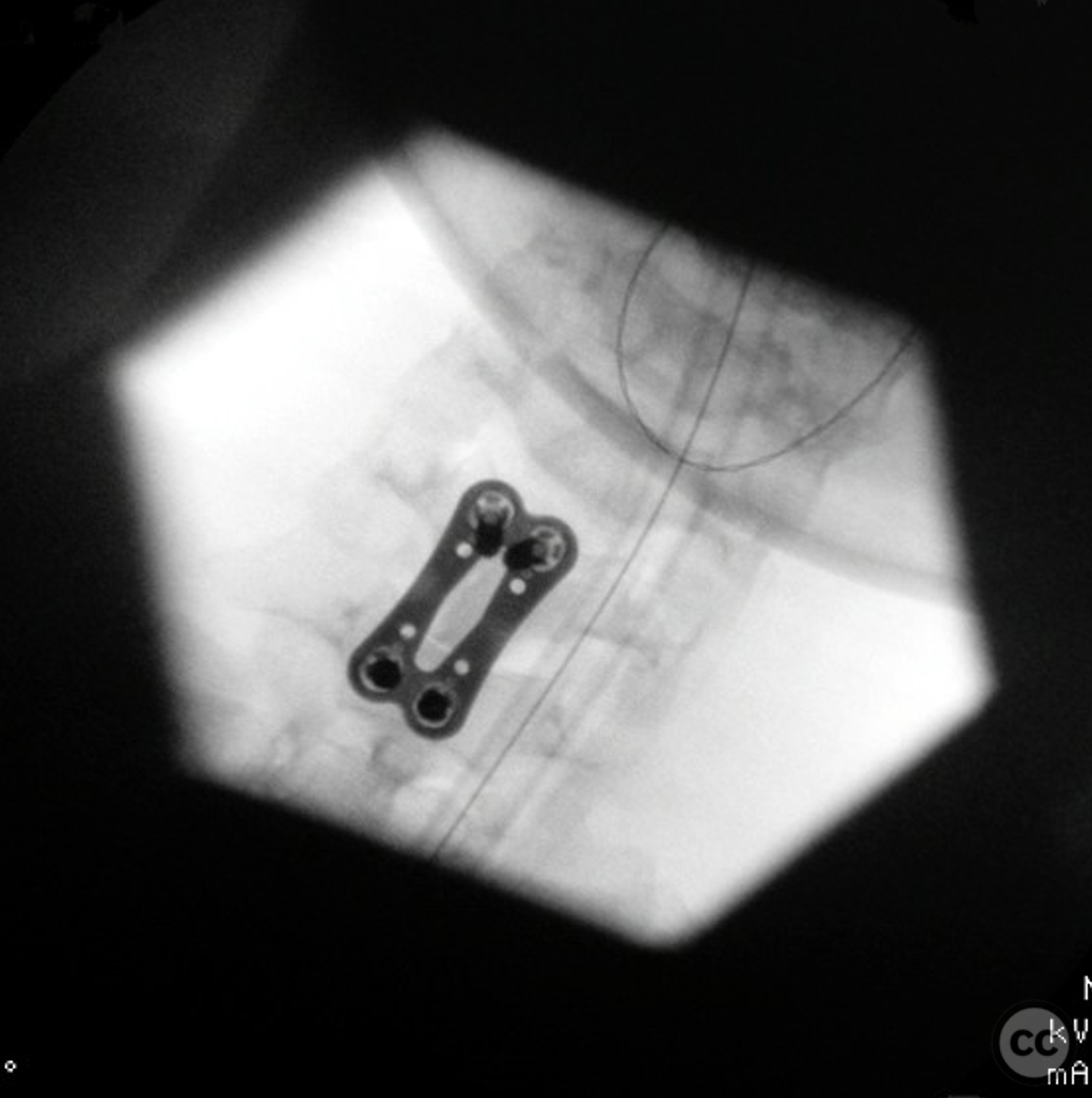
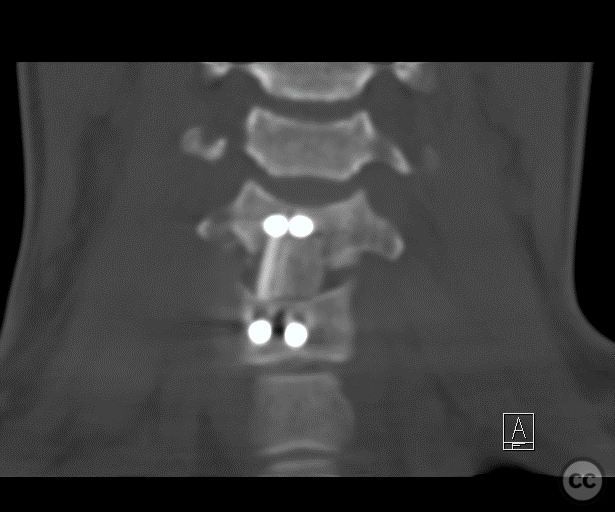
Operative remarks:Positioning did not reduce the injury by ligamentotaxis. Additional manouvre was indicated after exposure. Horizontal incision, classic Smith-Robinson-approach. Exposing from C5/6 to C7/Th1. Mounting a radiolucent Cloward retractor. As expected a ruptured ALL was visible above the teardrop fragment. As the upper part of C6 was not burst, decision was made to place the pin of the Caspar Distractor into C6, parallel to the upper endplate. Than the reduction was performed in two steps: First re-angulation of the vertebral bodies. Second the reduction of the traumatic slip C6/7 (retrolisthesis of C6 over C7) via the Caspar distractor pins. For the second part a special distractor was used that fixes each pin with a seperate set screw and pulls back the olisthetic vertebra (Trimline, Medtronic). After reduction a discectomy C6/7 and a partial (lower) corpectomy C6 was performed. A tricortical iliac crest graft was harvested, trimmed and inserted into the defect. After removal of the Caspar distractor the situation was judged as good enough for a monosegmental staililsation and fusion. A modern angle-stable plate was used for that (VECTRA, DePuySynthes).
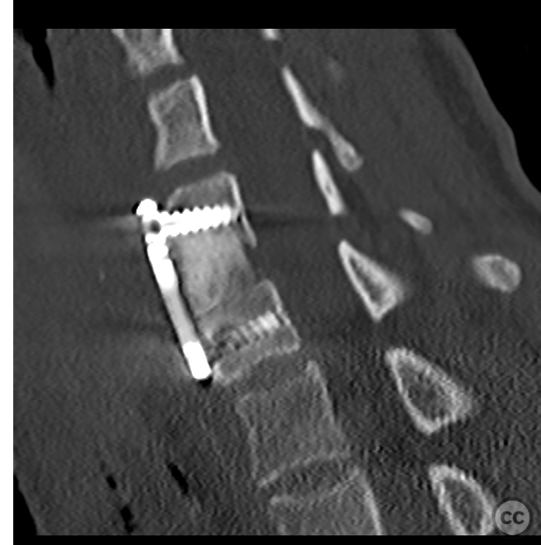
Postoperative protocol: Semirigid collar for 8 weeks. A soft collar for the nights. CT postop and X-rays to show appropriate reduction and congruence of the facets. If secondary loss of reduction would be oberved in lateral X-rays additinal posterior fixation would be recommended.
Follow up: No loss of reduction after 3 weeks and 8 weeks. Fusion visible on X-Ray after 3 month. A transient weekness of C7 left was present (M4) postop, but full strength was restored after 3 month. Slight loss of cervical lordosis at 2 year FU and degeneration of C5/6 while the patient remained asymptomatic.
Orthopaedic implants used: Anterior cervical plate system VECTRA cervical plating system (DePuySynthes)
Author's Resources & References
Search for Related Literature
Alexander Tapio Mameghani
- Switzerland , Argovia
- Area of Specialty - Spine
- Position - Head of Department

Industry Sponsership
contact us for advertising opportunities
User Discussion (2)
Guest User
Great case!
Dr Ed Oates
Fantastic reduction sequence capture. And excellent fusion (and clinical) outcome. Nice!