

Pediatric Elbow Dislocation with Medial Epicondyle Fracture
Score and Comment on this Case
Clinical Details
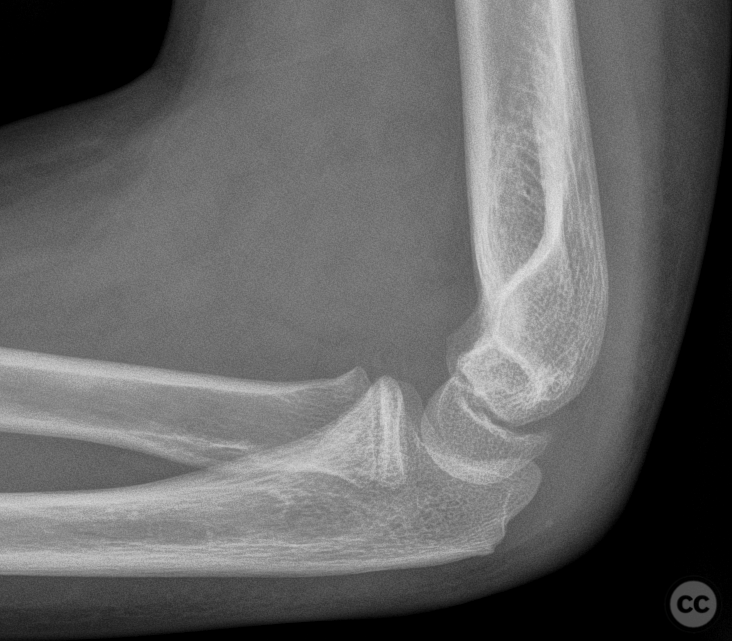
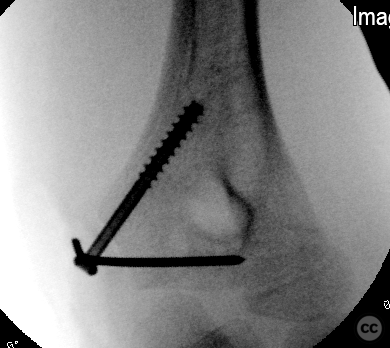
Clinical and radiological findings: An 11-year-old male presented after a fall from a 2-meter height onto an outstretched arm. Clinical examination revealed gross posterolateral instability of the elbow with spontaneous dislocation evan at 90 degrees of flexion. Radiological assessment confirmed the presence of a displaced medial epicondyle fracture without significant identifiable injury to the radial head, coronoid, capitellum, or trochlea.
Preoperative Plan
Planning remarks: The surgical plan was to achieve stable reduction of the elbow dislocation and medial epicondyle fracture. Suspicion of a TRASH lesion was high.
Surgical Discussion
Patient positioning: The patient was positioned supine with the arm on an arm table, facilitating access to the medial side of the elbow.
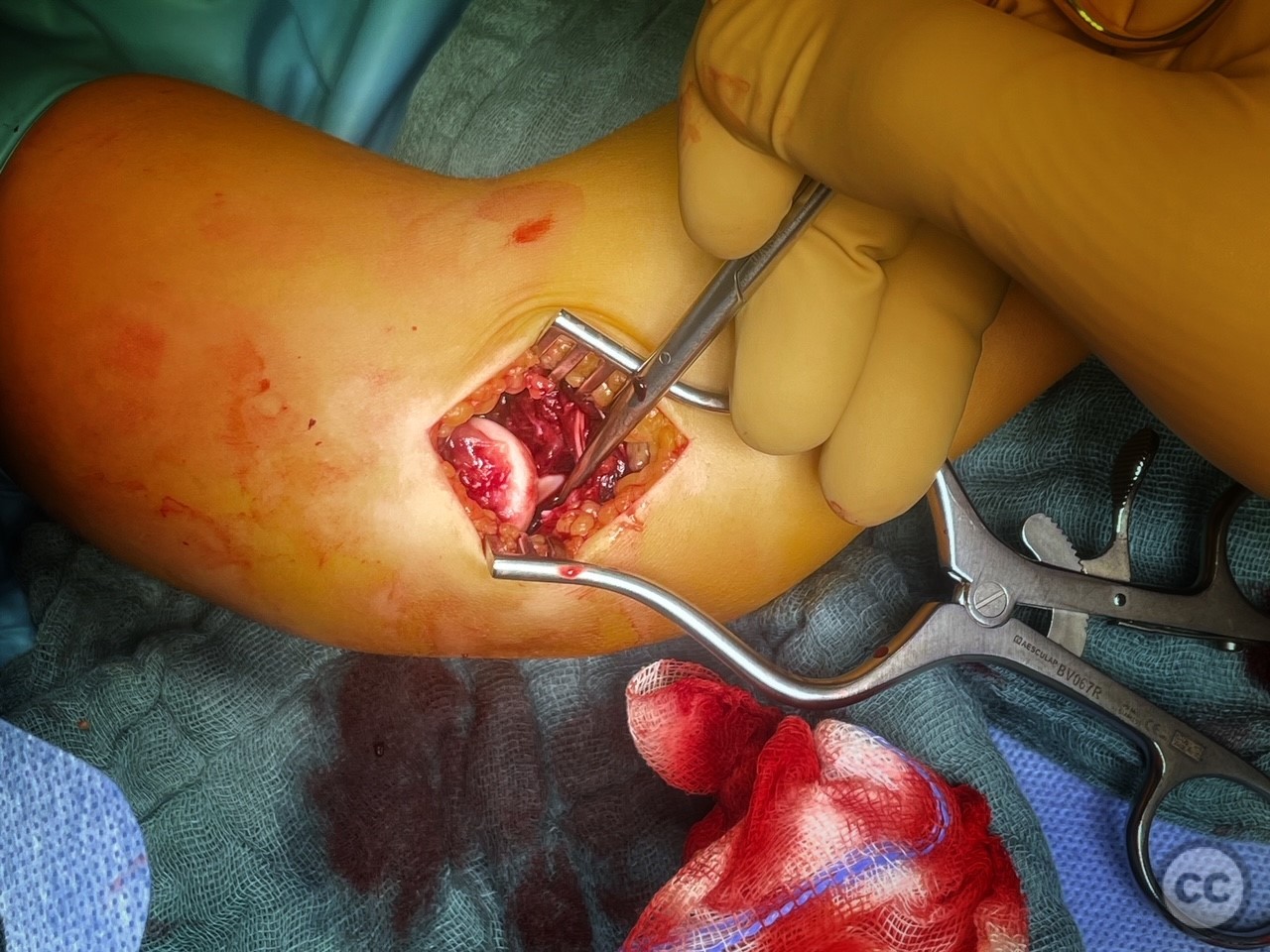
Anatomical surgical approach: A curved incision was made over the medial epicondyle, followed by subcutaneous dissection. Upon reflection of the displaced medial epicondyle fragment, a posterolateral dislocation of the ulna was noted. The approach allowed for direct visualization of the fracture, a complete anterior capsule rupture, near-complete rupture of the brachialis muscle, and identification of small osteochondral fragments from the coronoid process.
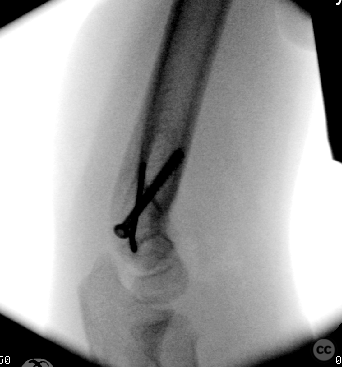
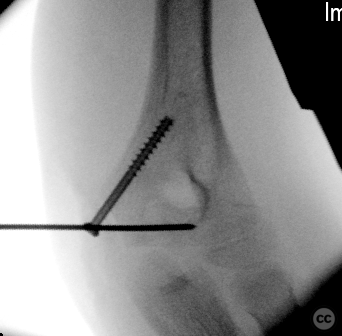
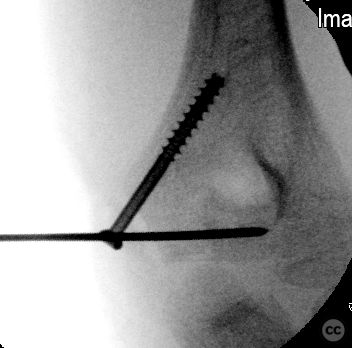
Operative remarks:Intraoperatively, concerns included managing the gross instability of the elbow and addressing multiple soft tissue injuries including the brachialis rupture. The anterior joint capsule was sutured, whilst brachialis was simply passively adapted through joint reduction and closure of the joint capsule. Along with the reattachment of the medial epicondyle fragment using a cannulated screw and K-wire fixation, this was sufficient to restore stability through a complete ROM. The ulnar nerve was identified and preserved throughout the procedure. Despite the complexity of injuries, and loss of medial collateral ligament integrity, a stable elbow joint was achieved.
Postoperative protocol: Postoperative rehabilitation included immobilization in an above-elbow fibreglass splint for 3 weeks to protect the repair and allow for secondary healing of soft tissue injuries.
Follow up: Not specified.
Orthopaedic implants used: retrograde 4.0 mm cannulated screw up the ulnar column, 1.6 mm K-wire in a transcondylar orientation
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 779 times
28 Feb 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Pediatric Elbow Dislocation with Medial Epicondyle Fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 38632840 Published Online Feb 28 2024.