






Two window posterolateral approach to Frosch Zone PLL/PLC
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: This is a 35-year old man following a fall from a a domestic height who sustained a left-sided posterolateral tibial plateau injury. The preoperative CT scans show isolated depression focused in the posterolateral corner with a majority of cortical depression and instability occurring in the poster aspect of the plateau postreria to the fibular head. There was no indication of concomitant ligamental injury. Preoperative planning and assessment of the three-dimensional reconstructions suggested that a classical anterolateral approach would not provide adequate exposure or visualisation of the posterolateral plateau. More so so fix station hardware brought in from the anterolateral aspect or in an anteroposterior fashion would be unlikely to adequately capture and stabilise the postcode area only fragments. The plan was to to buttress post you really using a too working window with the option of of extending this approach with a lateral epicondyle osteotomy should reduction and visualisation prove difficult.
Preoperative Plan
Planning remarks:
Surgical Discussion
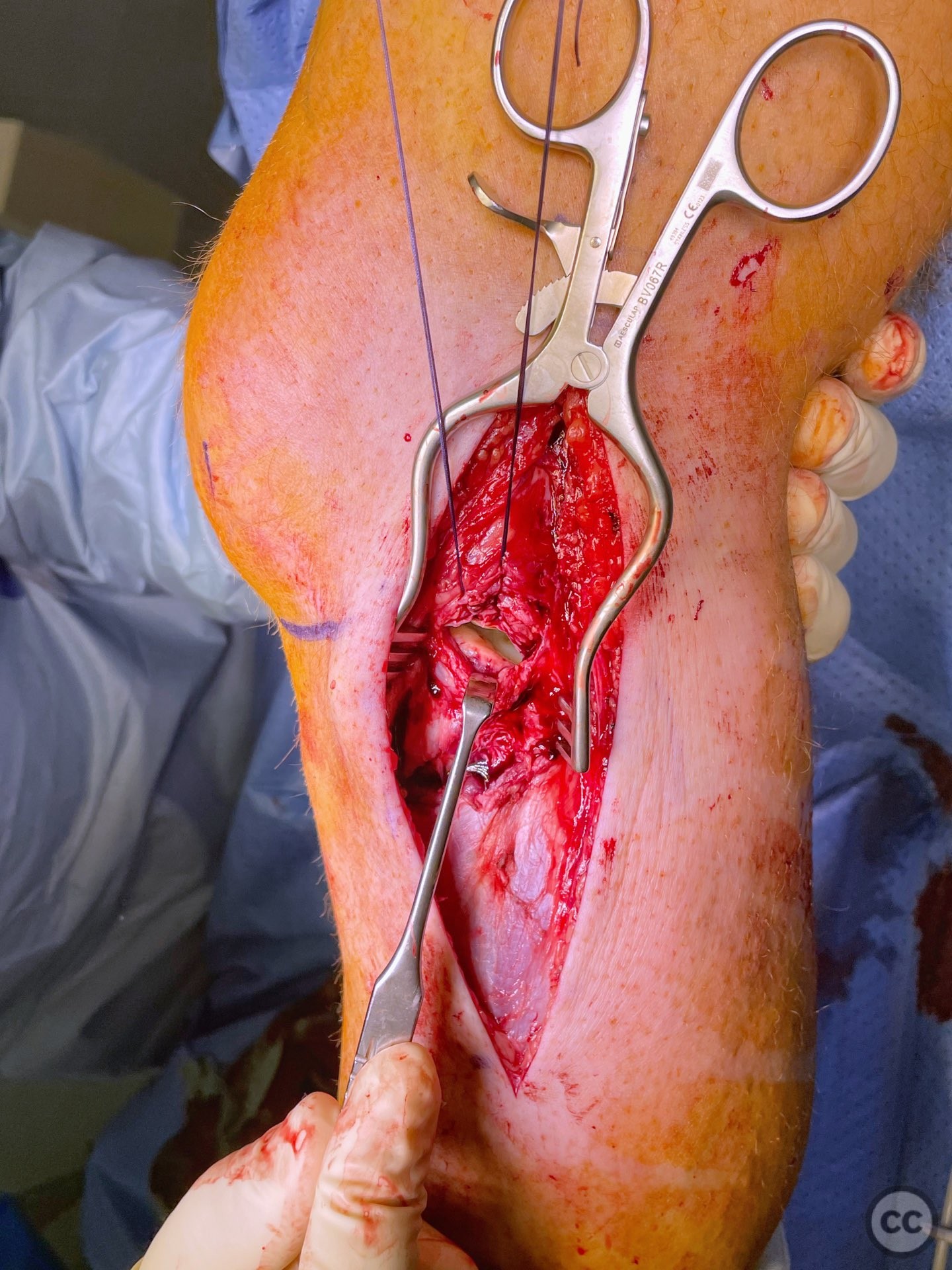
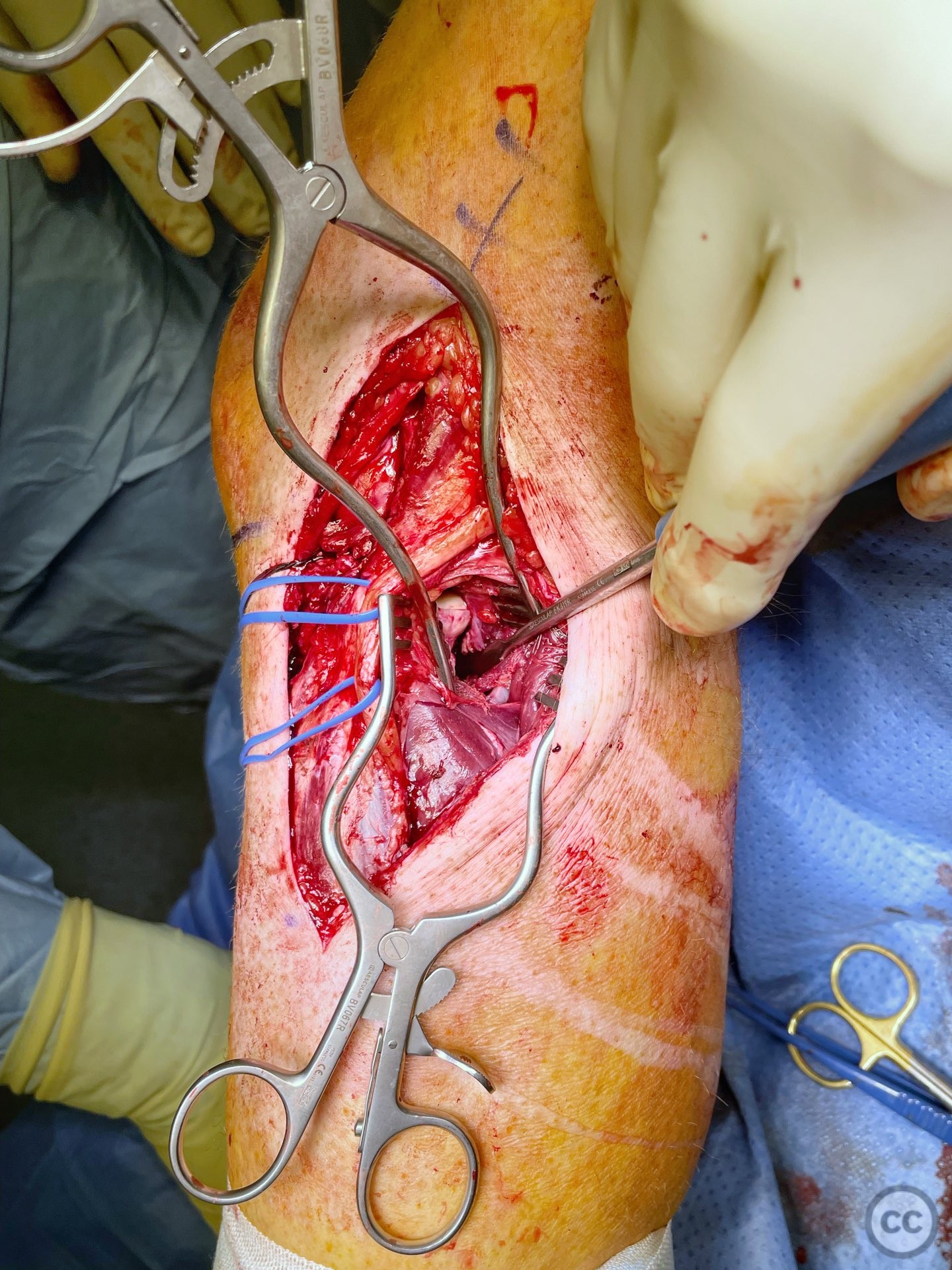
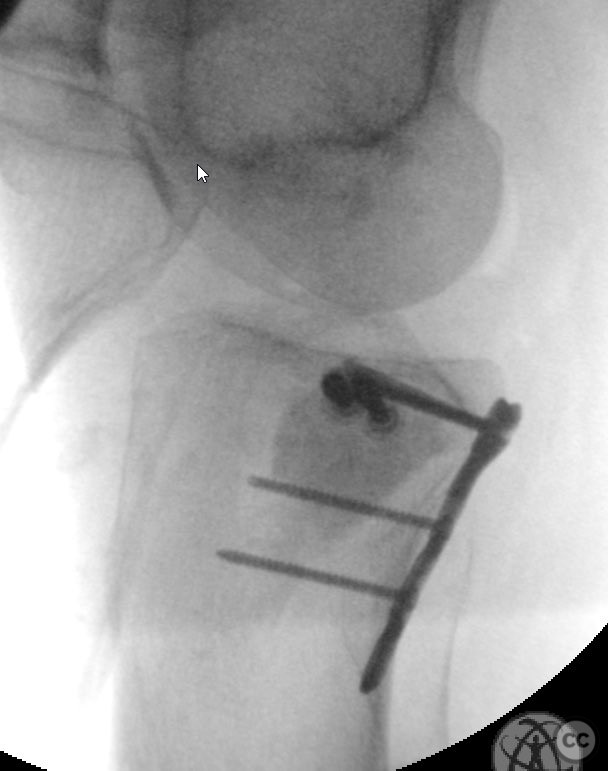
Operative remarks:Operation was performed around 10 to 14 days post injury following subsidence of post-operative swelling. Patient was placed in a simile lateral position within me Drake freely and a carbon roll placed under the medial aspect of the distal allowing the link to fall into varus. A direct lateral incision was made over the fibula head and lateral epicondyle as indicated in the attached images. To working windows for established one 1-in the classical anterolateral position with sub meniscal arthrotomy demonstrating a limited view of the the lateral tibial plateau. A second window was created posteriorly. This window is between the poster aspect of the biceps tendon and peroneal nerve and the medial head of gastrocnemius. Careful dissection down to the post urea aspect of the joint line is achieved with proximal medial retraction of the Billy of popliteus. The lateral genicular artery was identified and preserved. Sharp debridement of the lateral aspect of solis from the bone was done offering good direct visualisation of the bony tibial joint margin. As can be appreciated from these intra-operative photos the working window is relatively small. Visualisation of reduction is difficult. Nonetheless we achieved an anatomical reduction of the joint depression, and filled the the defect with hello plastic bone replacement material. The atukula surface was rafted with two 4.0 mm cannulated screws and then buttressed posteriorly with a modified 2.7 mm distal radial t plate. The the long limb of the t plate needs to be placed carefully distally taking into consideration the fibrous arch of soleus and the branching of the popliteal artery into the anterior or posterior tibial arteries passing through this region.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 2543 times
22 Dec 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Two window posterolateral approach to Frosch Zone PLL/PLC. Journal of Orthopaedic Surgery and Traumatology. Case Report 39519854 Published Online Dec 22 2022.