







Proximal Tibia Hyperextension Fracture in an Osteopenic Patient
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: A 65-year-old female with a history of alcoholism and multiple previous falls presented with a hyperextension injury to the right proximal tibia. Radiographs and CT scans revealed a hyperextension fracture of the proximal tibial plateau, with approximately 10deg of anterior tibial tilt - classifiable as AO/OTA 41-A3 with B2 component. The patient exhibited marked osteopenia.
Preoperative Plan
Planning remarks: The preoperative plan involved a limited anterolateral incision to address the fracture. The approach aimed to expose the anterolateral tibial cortex, reduce the anterior step-off, and restore the posterior tibial slope through manipulation of the entire joint block.
Surgical Discussion
Patient positioning: The patient was positioned supine on a radiolucent operating table with the right knee flexed to approximately 30 degrees over a carbon fiber roll, supporting the distal aspect of the thigh. A tourniquet was applied to the proximal aspect of the ipsilater
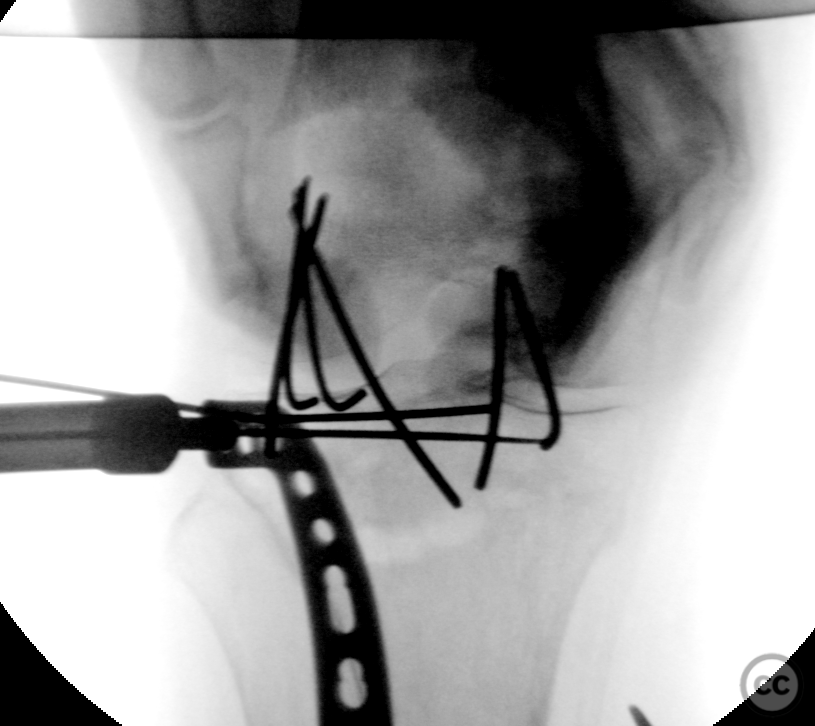
Anatomical surgical approach: A longitudinal incision was made over the lateral aspect of the joint line. The iliotibial tract fibers were identified and split to the level of Gerdy's tubercle. Subperiosteal elevation of the iliotibial fibers from Gerdy's tubercle was performed, along with splitting of the proximal aspect of the fascia of tibialis anterior, exposing the anterolateral tibial cortex. Subperiosteal dissection continued anteriorly to the level of the patellar tendon. A submeniscal arthrotomy in the anterior aspect demonstrated an intra-articular anterior step, which was reduced through direct manipulation and secured with two anterior-to-posterior Kirschner wires (K-wires). Mobilization of both medial and lateral plateaus en bloc was performed to reduce anterior tibial tilt. Multiple 2.0 mm K-wires were introduced from anterior to posterior, engaging both medial and lateral plateaus. A broad osteotome was used to facilitate sequential levering of the proximal joint, restoring approximately zero to five degrees of posterior tibial tilt.
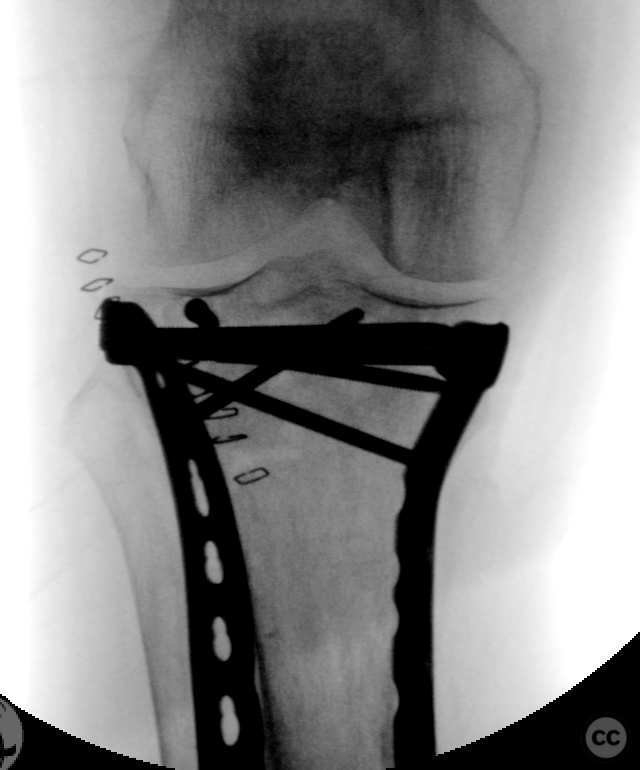
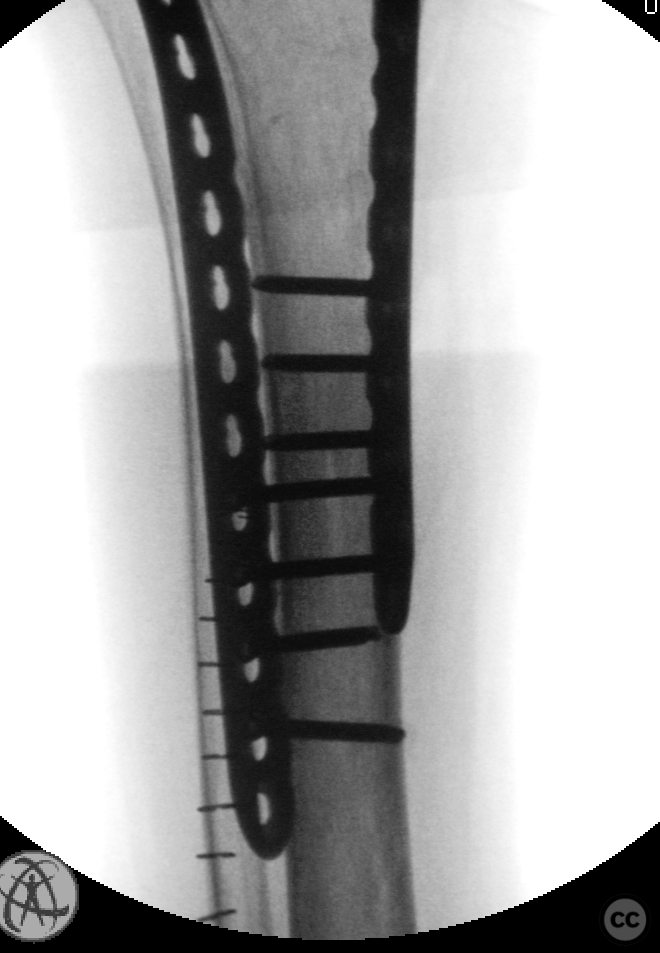
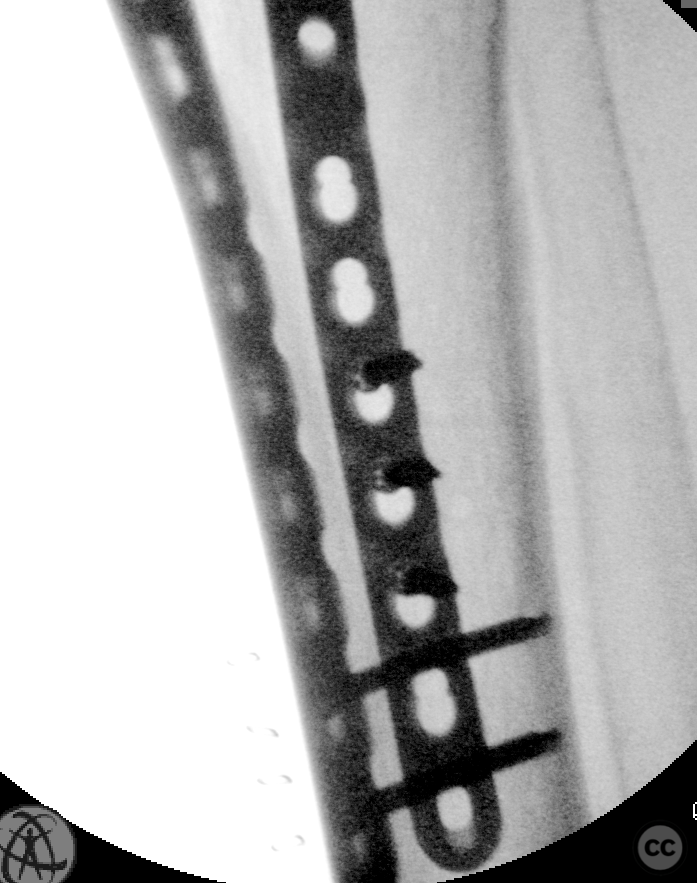
Operative remarks:The bone substance at the anterior aspect of the tibial articular surface was very soft, making primary screw fixation poor. Therefore, two anterior-posterior K-wires were left in position pending later plate osteosynthesis of the lateral tibial plateau. Minimally invasive installation of a long 3.5 mm proximal lateral tibial plate bent to conform to the anterolateral cortical contour followed. This plate was secured distally with a single 3.5 mm cortical screw. Through active reduction maneuvers over in situ K-wires, four locking screws were introduced into subchondral bone from the anterolateral side, securing restoration of posterior tibial tilt. A limited medial longitudinal incision provided access for minimally invasive insertion of a medial 3.5 mm plate, which was secured with bicortical screws distally and four 4.0 mm proximal locking screws engaging the joint block proximally.
Postoperative protocol: Not specified
Follow up: Not specified
Orthopaedic implants used: Long 3.5 mm proximal lateral + medial tibial plates (Synthes)
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 350 times
03 Jul 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Proximal Tibia Hyperextension Fracture in an Osteopenic Patient. Journal of Orthopaedic Surgery and Traumatology. Case Report 41994082 Published Online Jul 03 2024.