.png)














Ipsilateral plateau-shaft fracture
Score and Comment on this Case
Clinical Details
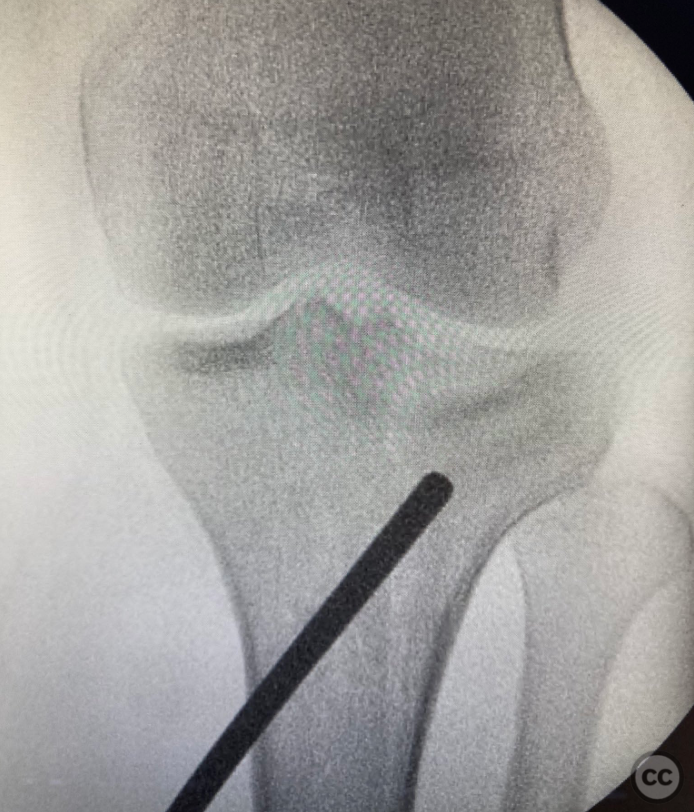
Clinical and radiological findings: Young man; low velocity motorbike accident. Isolated injury to leg. Closed fracture. Soft compartments. XR reveals a split depression lateral plateau fracture, with split extending down towards a proximal 1/3 shaft fracture with a large spiral wedge. CT scan reveals area of depression, displacements and additional undisplaced fracture lines, including a posterolateral wall and tuberosity.
Preoperative Plan
Planning remarks: Planned for internal fixation. Address plateau and shaft separately. Young patient with good bone; large depressed fragment thought suitable for elevation and rafting, plateau split not very 'blown out', so amenable to compression screws (without buttress). KIng tong clamp to restore condyle width. Look after undisplaced fracture lines to avoid displacement. IM nail for the shaft element.
Surgical Discussion
Patient positioning: Supine
Anatomical surgical approach: Percutaneous elevation and rafting/compression screws. Suprapatellar IM nail.
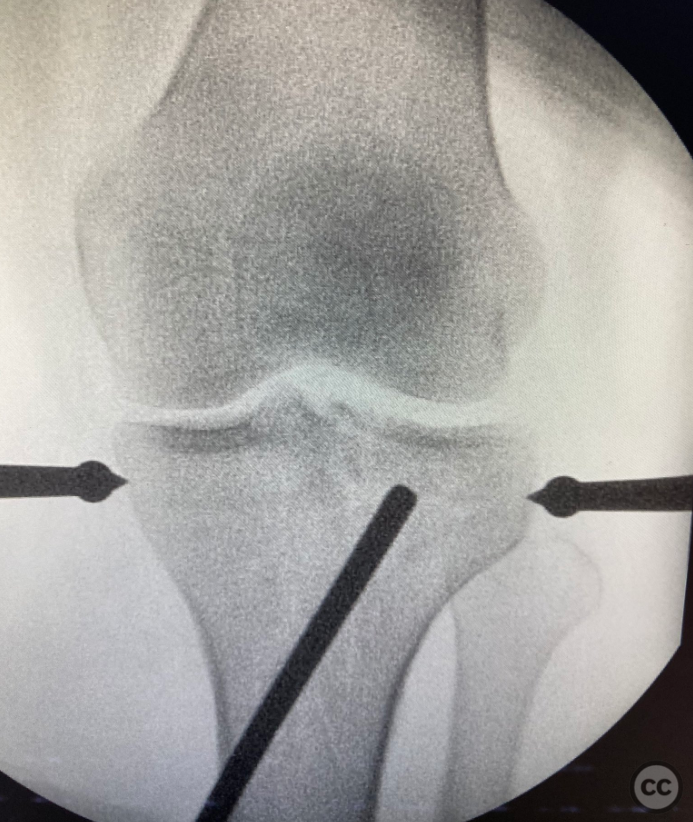
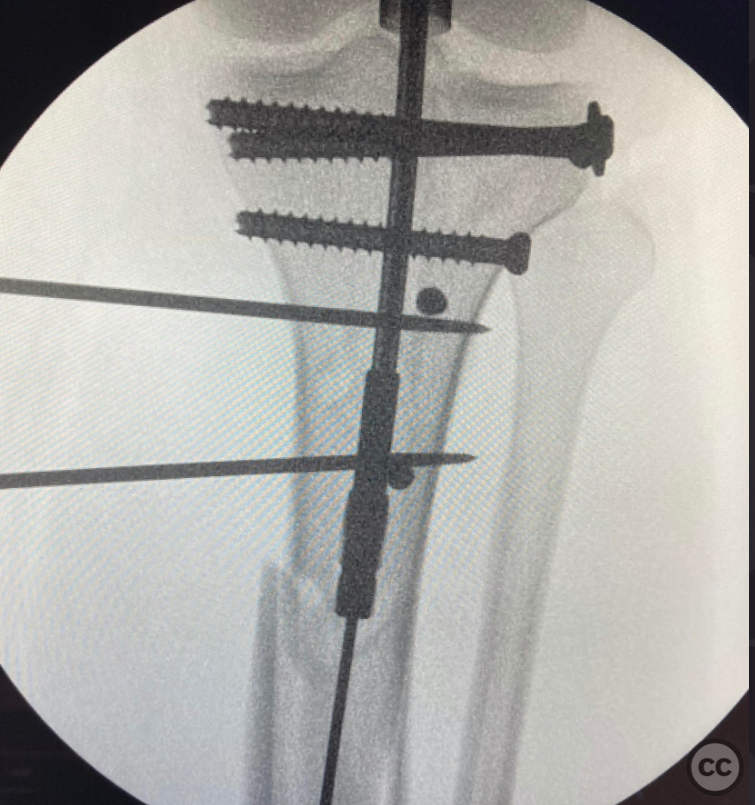
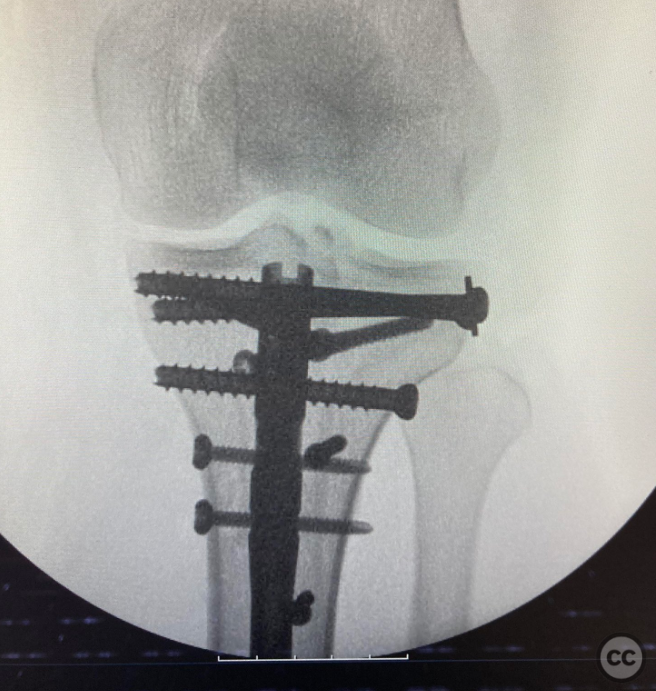
Operative remarks:Several ways of treating this injury, including in addition to what we did, long plate fixation and circular fixator. We chose this construct for its minimally invasive technique and rigid internal fixation. The rafting/compression screws were placed posteriot to expected path of nail. The tuberosity/undisplaced fracture lines were stabilised with 3.5 positional screws next. Suprapatellar entry was anterior to desirable because the entry point was fractured. The guidewire kept escaping posteriorly, so we used two sequential blocking pins. Additional percutaneous pointed clamp assisted in reducing the large spiral wedge. Nail has multidirectional locks proximally to further hold the plateau together.
Postoperative protocol: Immediate active knee range. Non weight bearing mobilisation for 6 weeks. Then buid to full by 12 weeks.
Orthopaedic implants used: 6.5mm partially and fully threaded cannulated cancellous screws. 3.5mm fully threaded cortex and cancellous screw. IM tibial nail.
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
User Discussion (2)
Guest User
Excellent choice abd excision
And exicusion
Guest User
Work of art !