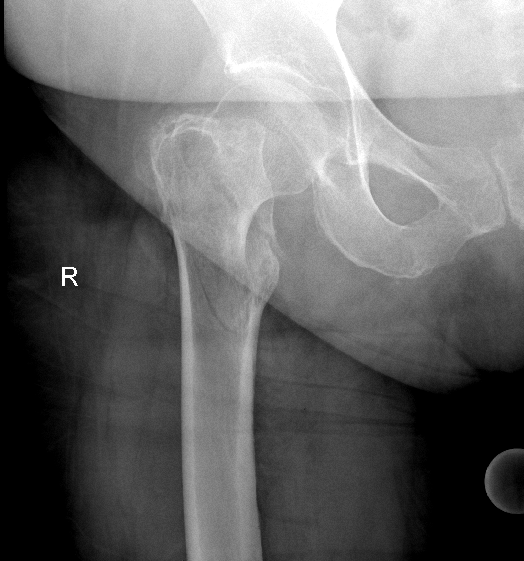




Comminuted subcapital and per/subtrochanteric femur fracture
Score and Comment on this Case
Clinical Details
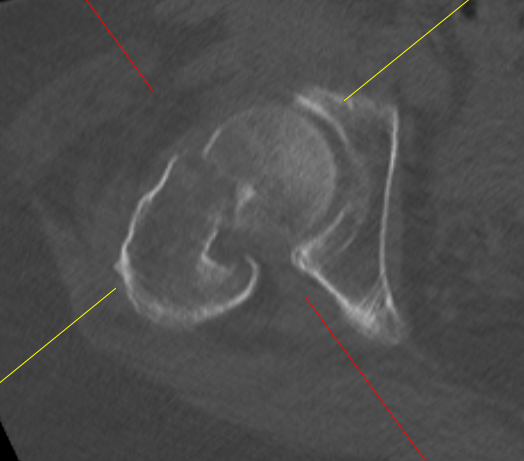
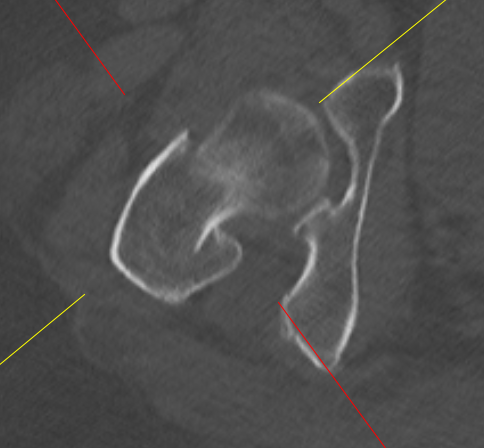
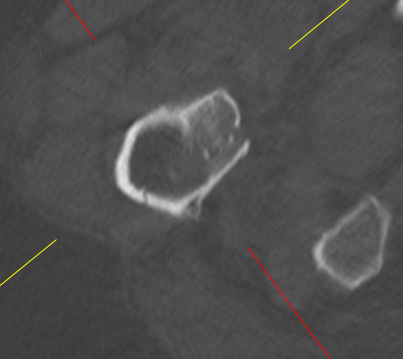
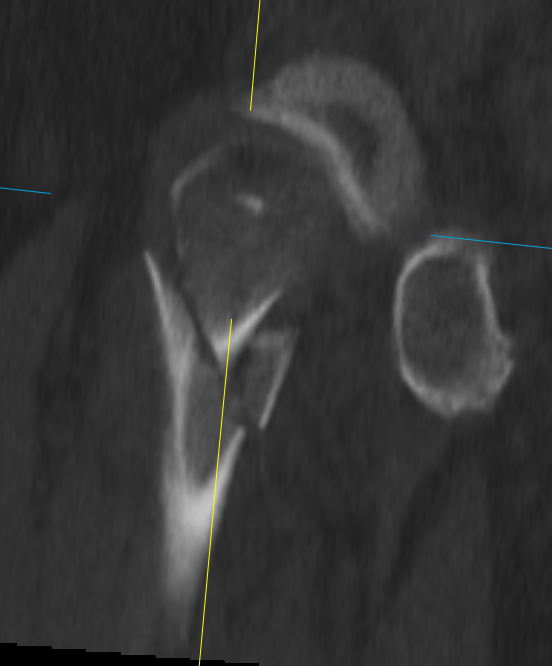
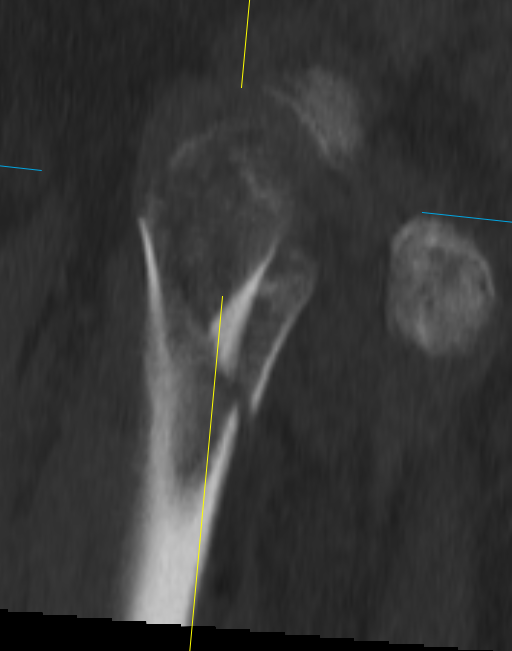
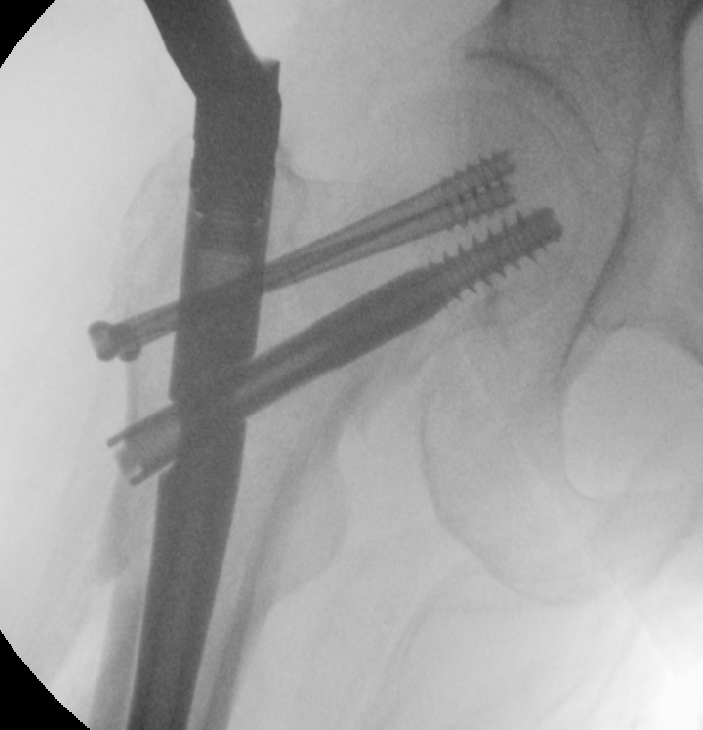
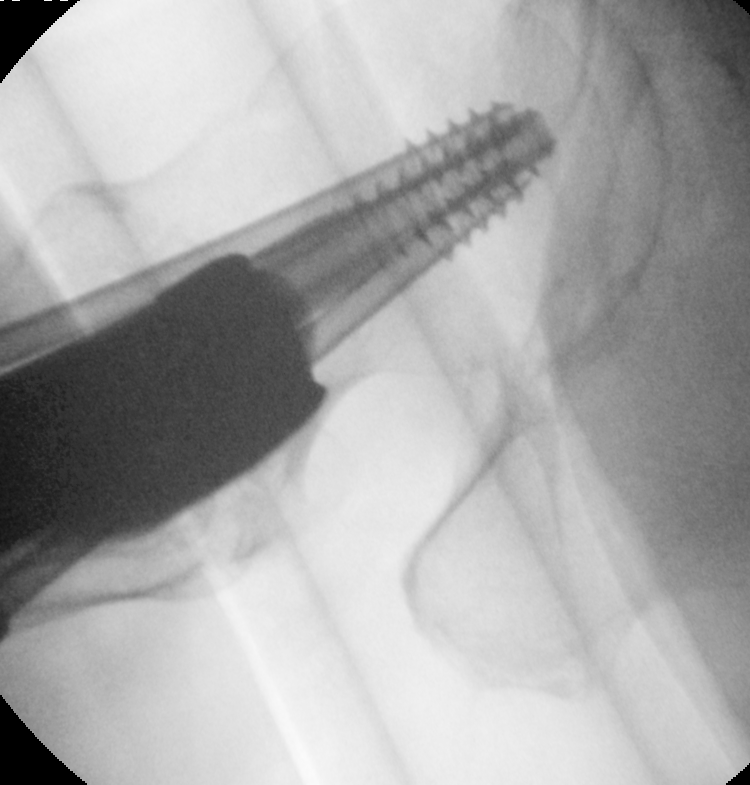
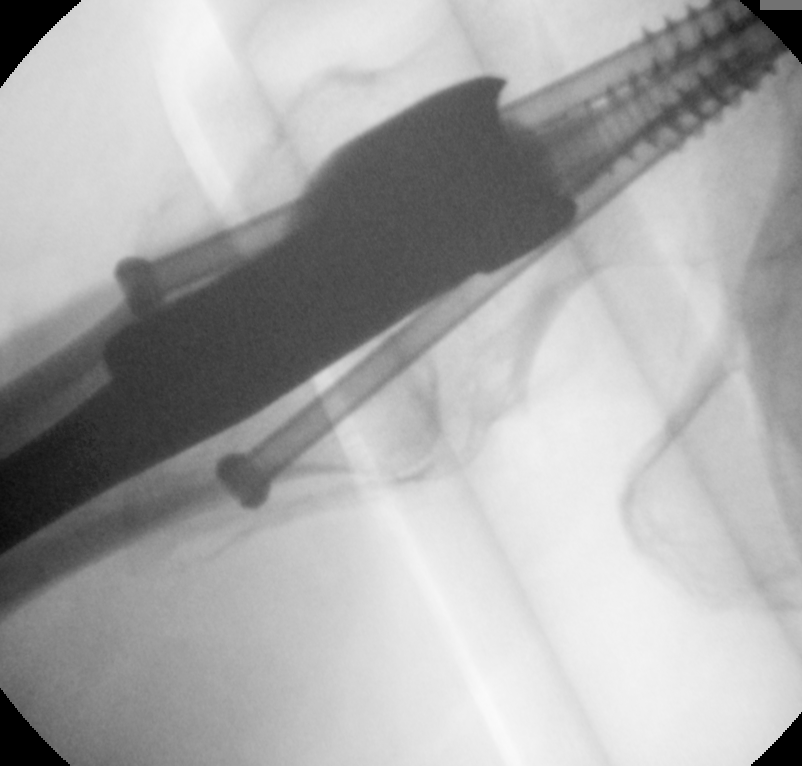
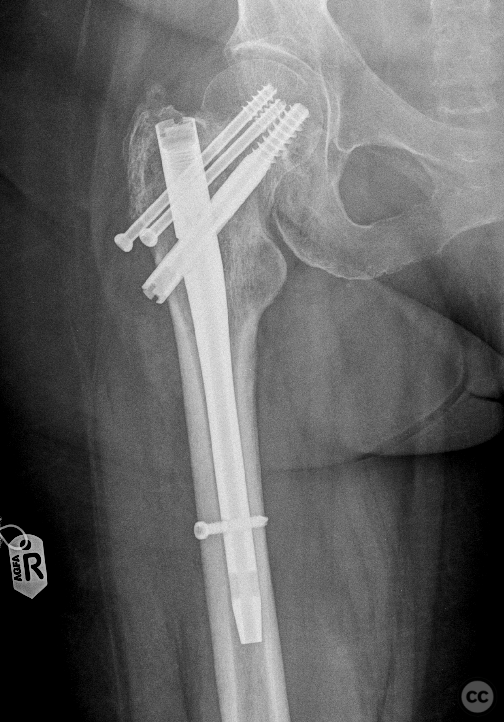
Clinical and radiological findings: This is a case of a 50-year-old female who sustained a domestic fall from a height of around 3 m onto hard flooring therby sustaining an isolated proximal right femoral fracture. The initial plain film radiographs suggested an inter-trochanteric fracture with some distal extension. The suspicion of a medial continuation of the intertrochanteric fracture into the subcapital intracapsular region was confirmed on CT. Thus this constellation represented a comminuted or even segmental proximal femoral fracture with both intracapsular and extracapsular components. The involvement of the sub/trochanteric region excluded arthroplasty as a primary management option. Due to limitations in available hardware a combined osteosynthetic plan involving intramedullary nail and adjuvant screw fixation was decided. The operation took place on a radiotranslucent traction table. A provisional reduction under traction was very successful. An open manipulation of the fracture was not required for adequate reduction. As a first step we proceeded with the introduction of the intramedullary nail and placement of the cephalomedullary-screw K-wire in a distal calcar position anticipating that more proximally in the head and neck adjuvent screw fixation would be required. Following placement of the distal K wire we then brought freehand anterior and posterior wires around the Gamma nail drill-jig entering the proximal lateral femoral cortex bypassing the nail and in a converging manner entering into bony substance of the femoral head. The two proximal wires were then drilledand measured and 2 cannulated 7.3 mm screws were brought in as anti-rotational fixation before the main cephalomedullary screw was drilled and placed. During implant insertion a small loss of reduction was noted copared to initial reduction films. This was not considered of such degree to warrant revision of osteosynthetic material. Unremarkable distal locking of the nail and removal of the drill guide followed. The postoperative management is initially conservative with maximum 20 kg weight-bearing for three weeks progressing to 50% weight-bearing in the subsequent three weeks. Full weight-bearing is anticipated following the sixth postoperative week.
Preoperative Plan
Planning remarks:
Surgical Discussion
Operative remarks:coming
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1183 times
17 Aug 2022
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2022). Comminuted subcapital and per/subtrochanteric femur fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 44958618 Published Online Aug 17 2022.