(Fictitious case!) Displaced Femoral Neck Fracture (31B2) in an Elderly Patient
Score and Comment on this Case
Clinical Details
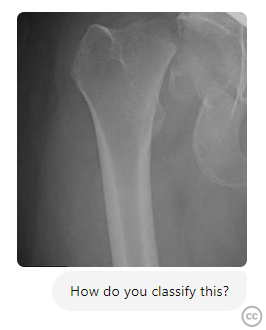
Clinical and radiological findings: An 82-year-old female presented following a low-energy fall at home. The patient, with a history of osteoporosis, reported immediate pain and inability to bear weight on the affected limb. Physical examination revealed shortening and external rotation of the right lower extremity. Radiographs confirmed a displaced femoral neck fracture, classified as AO/OTA 31B2. No other injuries were noted, and neurovascular examination was unremarkable.
Preoperative Plan
Planning remarks: The preoperative plan involved a direct lateral approach to the hip, aiming for open reduction and internal fixation (ORIF) using a dynamic hip screw (DHS) system. Given the patient's age and bone quality, this method was chosen to provide stable fixation and allow for early mobilization.
Surgical Discussion
Patient positioning: The patient was positioned supine on a fracture table with the affected limb in slight internal rotation to facilitate reduction. A radiolucent table was used to allow for intraoperative fluoroscopy.
Anatomical surgical approach: A longitudinal incision was made along the lateral aspect of the hip, centered over the greater trochanter. The fascia lata was incised in line with the skin incision, and the vastus lateralis muscle was split longitudinally to expose the lateral aspect of the proximal femur. Subperiosteal dissection was performed to visualize the fracture site. Reduction was achieved using traction and manipulation under fluoroscopic guidance.
Operative remarks:Intraoperatively, the fracture reduction was challenging due to comminution at the fracture site. Temporary fixation was achieved with Kirschner wires, followed by placement of a guide wire for the DHS. The lag screw was inserted into the femoral head, ensuring optimal positioning within the subchondral bone. The side plate was then attached to the femoral shaft, and additional screws were placed to secure the construct. Intraoperative fluoroscopy confirmed satisfactory reduction and fixation.
Postoperative protocol: Postoperatively, the patient was allowed toe-touch weight-bearing with a walker for six weeks to protect the repair. Physical therapy focused on range of motion exercises and gradual strengthening of the hip abductors. Full weight-bearing was anticipated by three months post-surgery, contingent on radiographic evidence of healing.
Follow up: Not specified
Orthopaedic implants used: Dynamic Hip Screw (DHS) system with a 135-degree side plate and 4-hole configuration.
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 220 times
07 Sep 2024
Add to Bookmarks
Full Citation
Cite this article:
Thomas Morscher. (2024). (Fictitious case!) Displaced Femoral Neck Fracture (31B2) in an Elderly Patient. Journal of Orthopaedic Surgery and Traumatology. Case Report 47694920 Published Online Sep 07 2024.