

















High-energy tibia and fibular fracture following a motorcycle accident
Score and Comment on this Case
Clinical Details
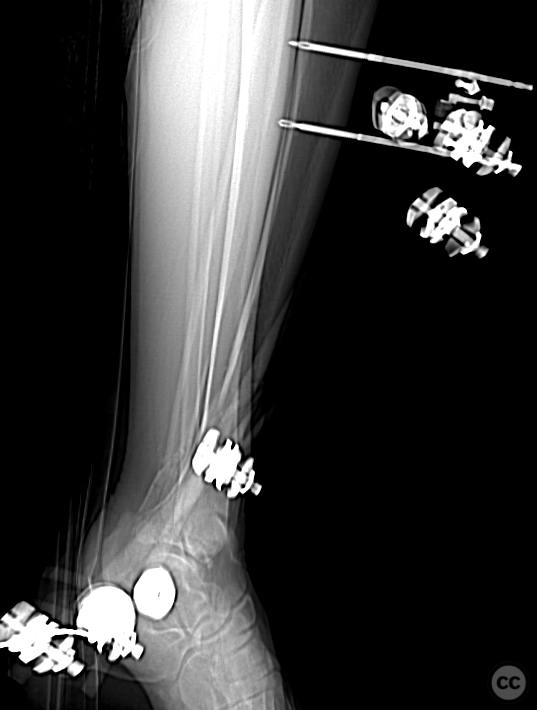
Clinical and radiological findings: A 32-year-old male presented after a motorcycle accident with significant closed soft tissue injury around the ankle. Initial plain films revealed comminuted fractures of the distal third of both the tibia and fibula. Subsequent CT imaging post-external fixation identified a comminuted tibial diaphyseal fracture extending into the metaphysis at the ankle joint, featuring large posterior and medial malleolar fragments and diaphyseal comminution. The fibula fracture was extensively comminuted from the syndesmosis region proximally. Soft tissue complications included large superficial necrosis over the lateral ankle and resolving fracture blisters medially.
Preoperative Plan
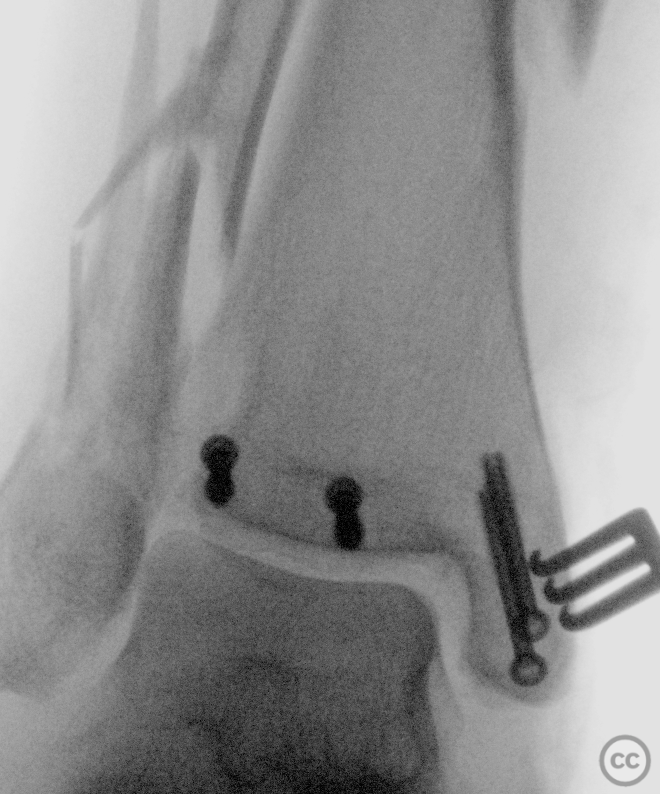
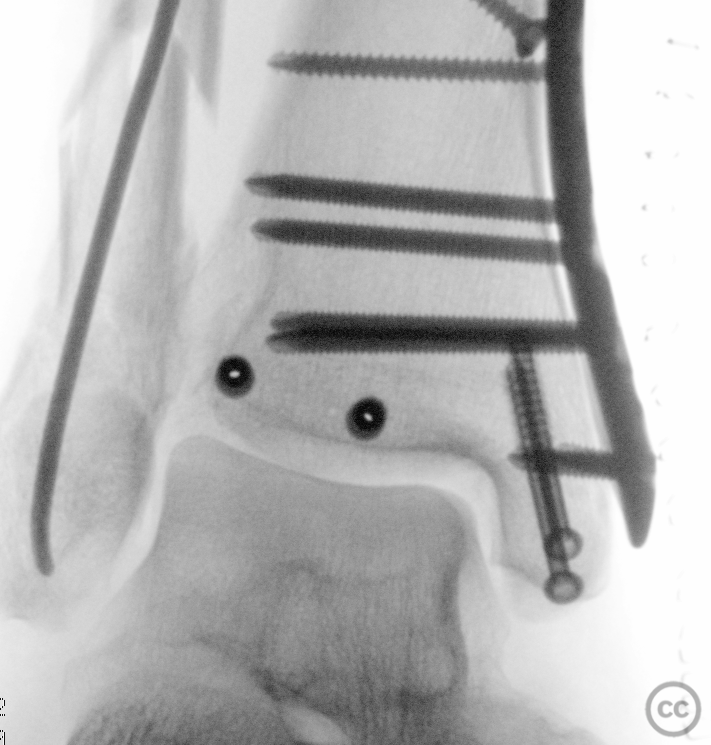
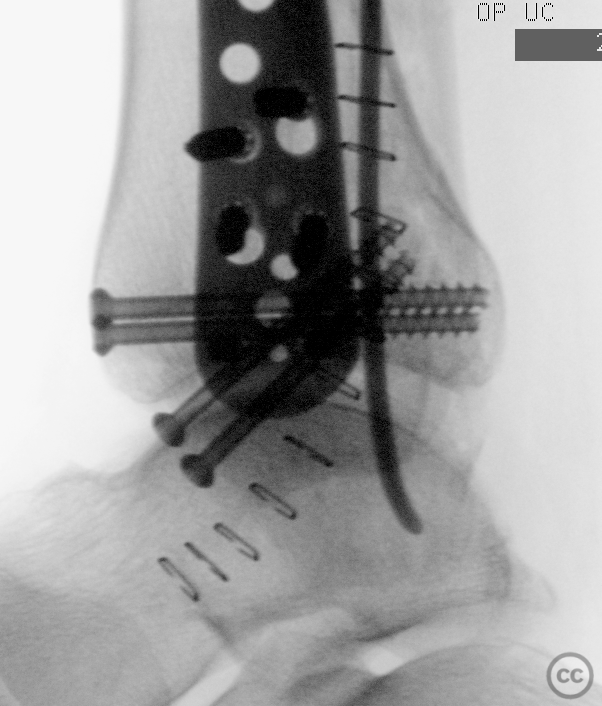
Planning remarks: The surgical plan aimed at fragment-specific screw fixation for the tibial fractures and minimally invasive plate osteosynthesis (MIPO) through a limited medial approach, avoiding direct lateral exposure due to soft tissue necrosis. For the fibula, percutaneous antegrade insertion of a 2.5mm titanium elastic nail was chosen to maintain axial alignment without directly addressing the lateral soft tissue injury.
Surgical Discussion
Patient positioning: The patient was positioned supine with the injured leg slightly elevated
Anatomical surgical approach: A limited medial approach was used for the tibia to directly address the medial malleolar fragment and allow for MIPO technique application. The posterior malleolar fragment was addressed through indirect reduction techniques. Percutaneous techniques were employed for fibular stabilization using a 2.5mm titanium elastic nail inserted antegrade, avoiding the compromised lateral soft tissues.
Operative remarks:The operative strategy was adapted to manage both the complex fracture patterns and the significant soft tissue injury. The decision against further syndesmotic fixation was made considering the satisfactory stabilization of the posterior syndesmosis and concerns over exacerbating soft tissue damage. The use of a titanium elastic nail for the fibula allowed for minimally invasive stabilization, respecting the soft tissue envelope.
Postoperative protocol: Postoperative rehabilitation included non-weight bearing mobilization in an ankle orthosis for six weeks, followed by a gradual return to weight-bearing as tolerated.
Follow up: Necrosis still resolving laterall at 10W (photo). RO TENS at 12weeks (fluro image)
Orthopaedic implants used: Fragment-specific screws for tibial fixation; MIPO Syntehs distal medial locking plate; 2.5mm titanium elastic nail for fibular stabilization.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 466 times
28 Feb 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). High-energy tibia and fibular fracture following a motorcycle accident. Journal of Orthopaedic Surgery and Traumatology. Case Report 47730808 Published Online Feb 28 2024.