









Lateral femoral condyle defect following GSW
Score and Comment on this Case
Clinical Details
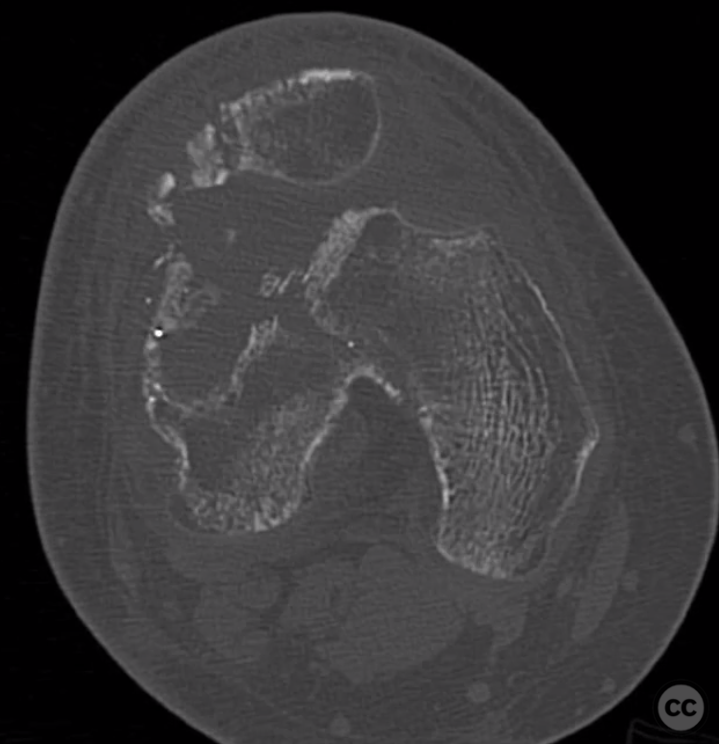
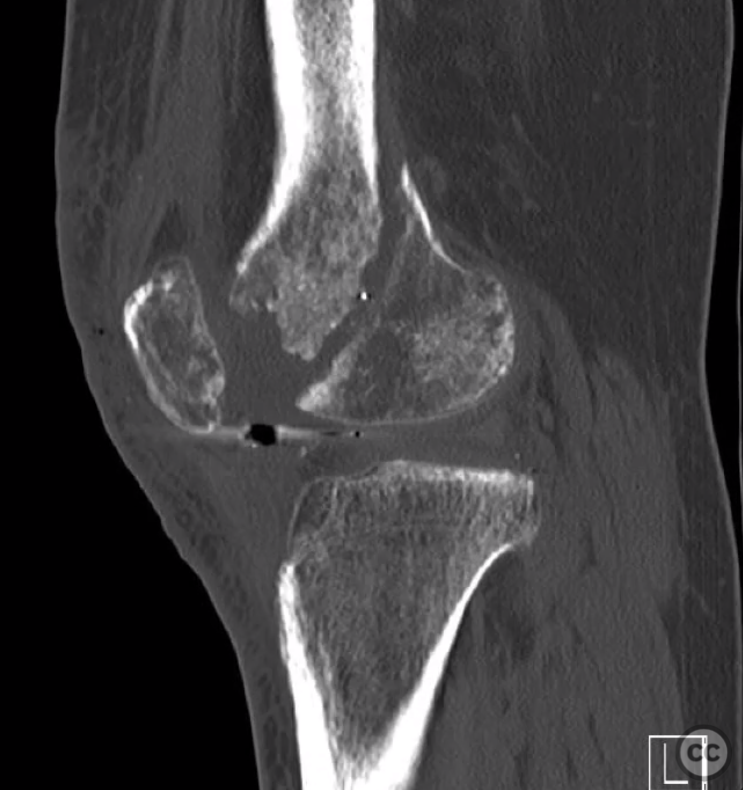
Clinical and radiological findings: 20yo male. Caught in crossfire, low velocity gsw. Seen at an outside hospital where he’s treated with neglect. Comes to me 7 months later with a healed wound, no history of infection. Moderate effusion. Knee rom 10-30. Very painful knee. He’s trying to get along with life. Can’t work. Can’t do much of anything given his knee situation. Problems: 1) knee stiffness (10-30). Arthrofibrosis + the fact that his patella is stuck in the lateral defect. 2) articular bone loss. It’s a big hole, but it’s not primary wb zone, mostly patellofemoral. 3) patellar subluxation. Problem mega. Combo of bony and soft tissue problems. 4) nonunion of lateral femoral condyle. Not a huge problem but needs to be addressed. 5) knee pain- sources? Patella stuck in defect, etc.
Preoperative Plan
Planning remarks:
Surgical Discussion
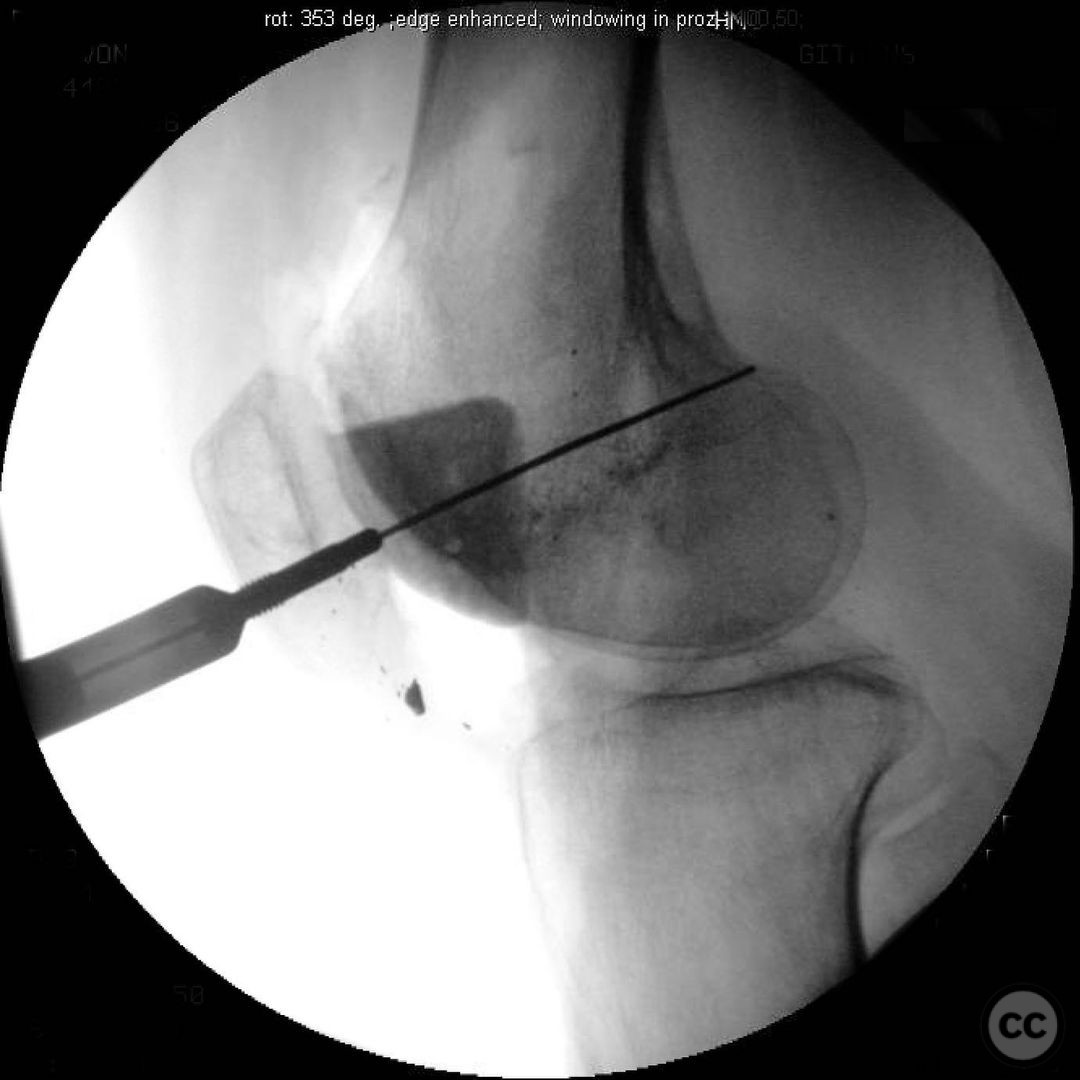
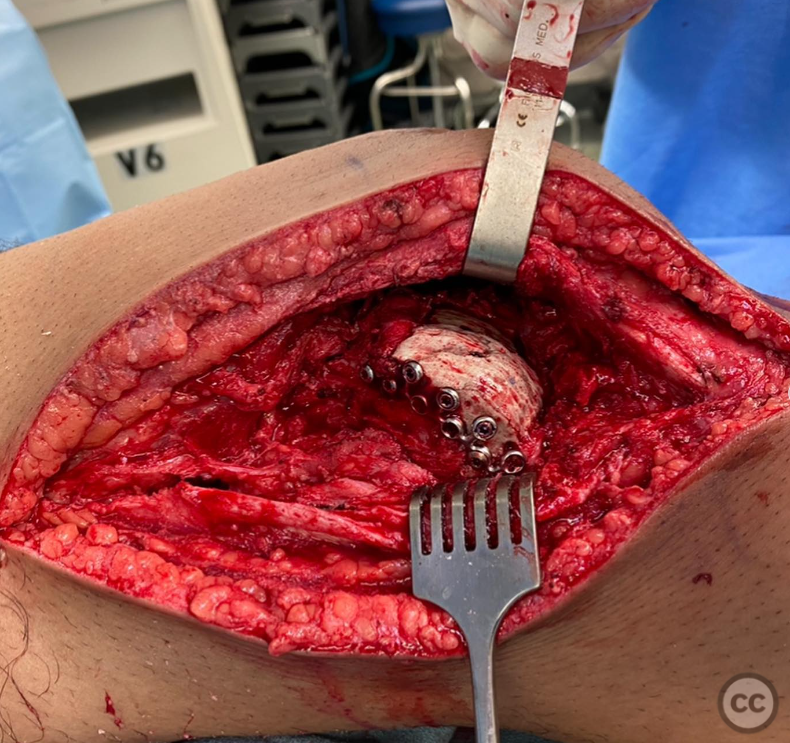
Operative remarks:Goal 1- motion. Needs an open LOA, possible quad-plasty, and most importantly-recreation of the trochlea, and some sort of soft tissue procedure to get the patella tracking properly. 2) nonunion- clean up and fix 3) osteochondral defect- best dealt with via anatomic osteochondral block allograft (takes a long time to match). Do you want to try to do these things all at once? The risk of failure of each is quite high. On top of that- based on how the patellar cartilage is- even if you do a perfect osteochondral grafting- is he still going to have debilitating patellofemoral pain? For these reasons, I think staged management is super important. For me this is a 2 stage operation with goal 1 being restore motion. Get the knee moving normally, patella tracking normally, and then reassess. That required mega releases, rebuilding the trochlea with pmma and a medial imbrication. Plan was to see how he does and convert to a fresh osteochondral allograft, but he freaking loves his cement trochlea too much to commit to stage 2. Eventually he will show back up, but since his last follow up I haven’t seen him.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1261 times
15 Jan 2023
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2023). Lateral femoral condyle defect following GSW. Journal of Orthopaedic Surgery and Traumatology. Case Report 48843770 Published Online Jan 15 2023.