





ECMES vs femur - its a long way to the top
Score and Comment on this Case
Clinical Details
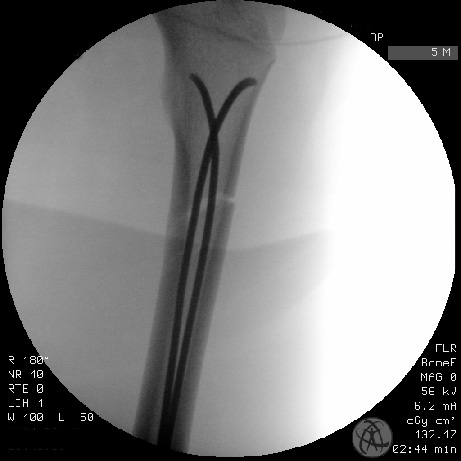
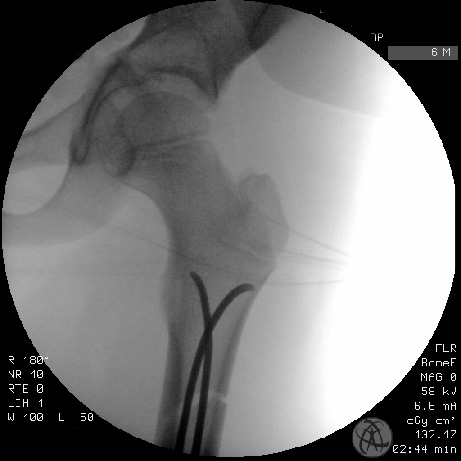
Clinical and radiological findings: This is the case of a 9yo boy who suffered a sledding injury - doubled on a sled with his older brother they collided with a tree at speed. The 9yo patient sustained multiple bony injuries including left femur and pelvis. We are discussing the left-sided proximal femoral shaft fracture in this case. As can be identified on the pre-operative plane film imaging, the leg was immobilized pre-hospital in a Thomas traction splint. There is an oblique fracture of the proximal femoral diaphysis with ~100% displacement, moderate angulation and minor non-displaced comminution. A closed and in neurovascularly intact injury we opted for an immediate operative stabilization of the fracture using closed reduction and intramedullary fixation using two 2.5mm ECMES titanium nails. The operation was done supine on the operating table with a freely draped left leg to the pelvic brim. The patient was positioned such on the table that fluoroscopy was not obstructed by metallic elements of the table structure. Medial and lateral supracondylar nail entry points were used and under manual traction, closed reduction was achieved allowing me to traverse the fracture with the ECMES. The two nails were pre-bent distally so as to cause bowing at the level of the fracture. Following introduction of both nails this bowing provided sufficient force across the fracture plane reducing it to near anatomical position.
Preoperative Plan
Planning remarks:
Surgical Discussion
Operative remarks:Firstly, I was pleased that this fracture was able to be reduced closed. Often with high energy femoral shaft fractures in children I find that there is often soft tissue blocking a closed reduction and I often have to open the fracture and reduce it directly. This was not the case here and the resulting and anatomic reduction is very satisfying. My only criticism in this case is perhaps the choice of the 2.5 mm titanium nails, which look a little anorexic given the diaphyseal width. I find it difficult enough entering the medial and lateral distal femoral cortices, turning the hard corner into the canal and then driving the nails proximally into the proximal femoral metaphysis. This involves an awful lot of hammering, and the multiple bends in the nail absorb a lot of energy which is otherwise meant to drive the nail forwards. In this case the nails simply didn’t carry the energy to allow the driving of the nails further proximally into the cancellous region of the trochanter or calcar. Whether a 3 mm nail would have improved ability to drive things further proximately I am uncertain. I am however certain that it would require more swearing. Either way, in this case the 2.5 mm nails were anchored securely and have provided adequate stabilization of the anatomically reduced fracture..
Orthopaedic implants used: ECMES 2.5mm titanium intramedullary nail
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 2350 times
20 Mar 2021
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2021). ECMES vs femur - its a long way to the top. Journal of Orthopaedic Surgery and Traumatology. Case Report 48844067 Published Online Mar 20 2021.