















Multifragmentary Proximal Humerus Fracture with Scapula Fracture in a Polytrauma Patient
Score and Comment on this Case
Clinical Details
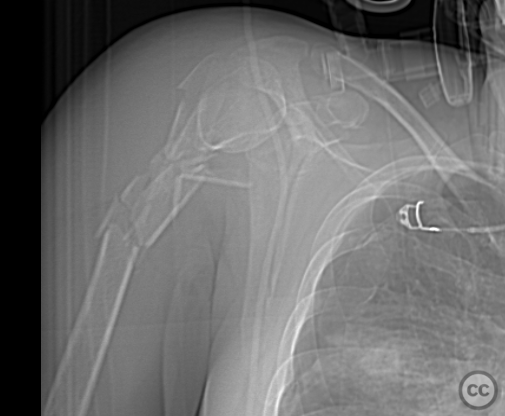
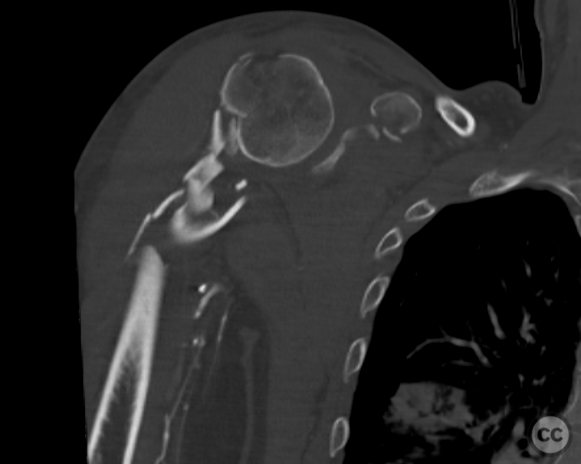
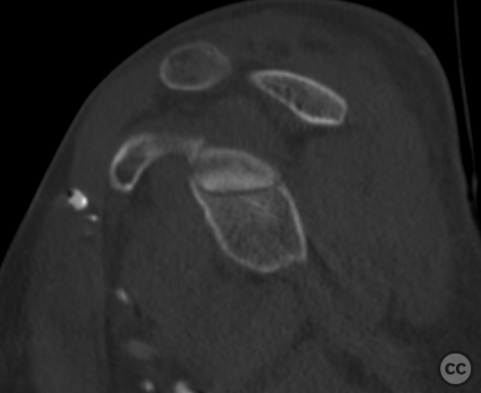
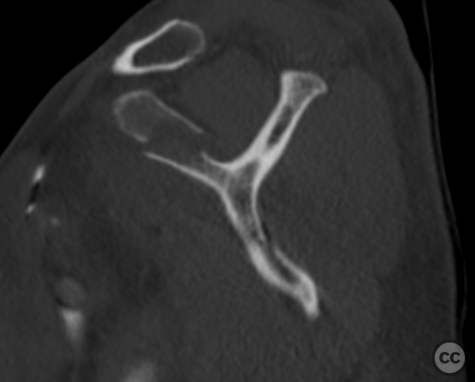
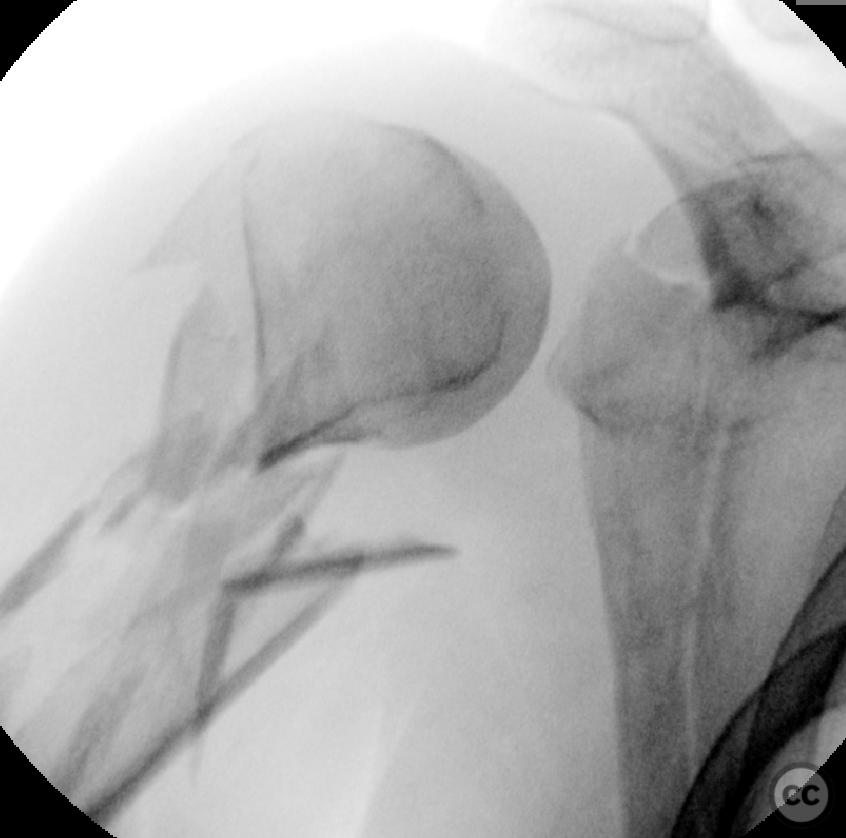
Clinical and radiological findings: A 38-year-old female involved in a motor vehicle accident presented as a polytrauma including multiple extremity injuries. Among these was a closed multifragmentary proximal humerus fracture associated with a scapula fracture, notably a displaced superior glenoid fracture involving approximately 25% of the glenoid with extension into the acromion and the scapular neck radiating to the inferior angle. Initial management focused on polytrauma stabilization with simple limb immobilization.
Preoperative Plan
Planning remarks: The definitive surgical plan, executed approximately 10 days post-injury, aimed to address the proximal humerus fracture using a bridging plate technique while attempting limited fixation of the glenoid component through the same surgical window, avoiding a dedicated dorsal approach to the scapula.
Surgical Discussion
Patient positioning: The patient was positioned in a beach chair position.
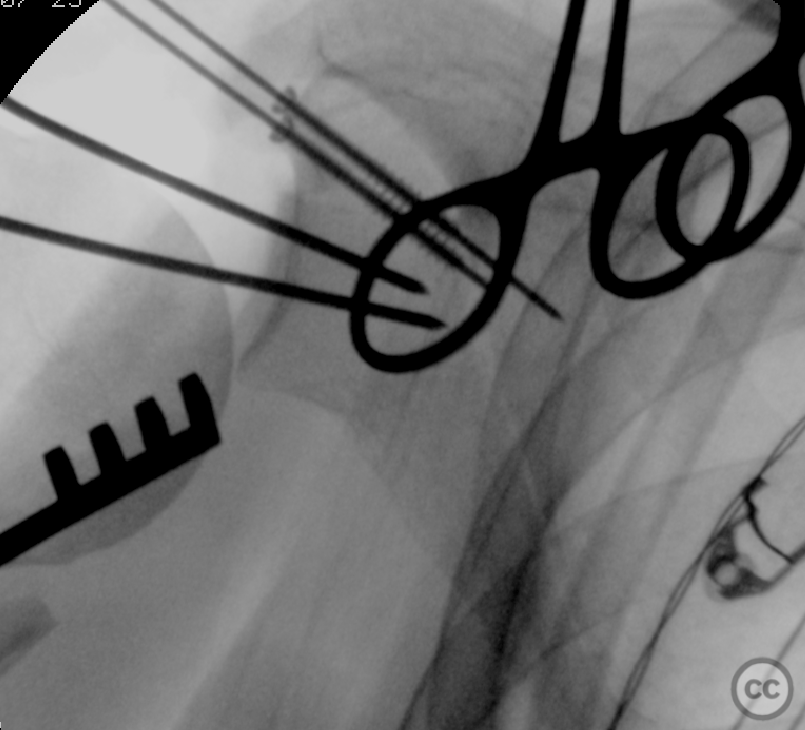
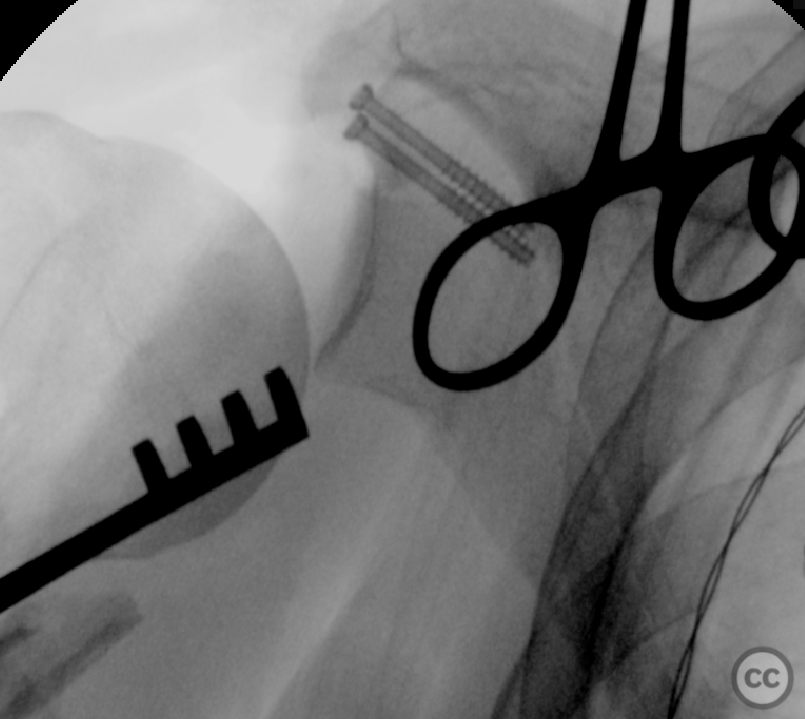
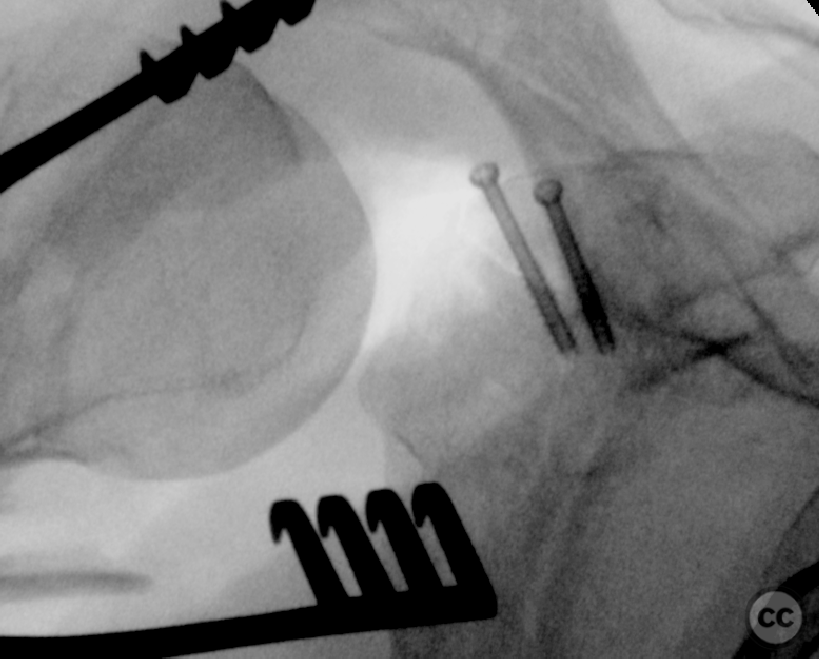
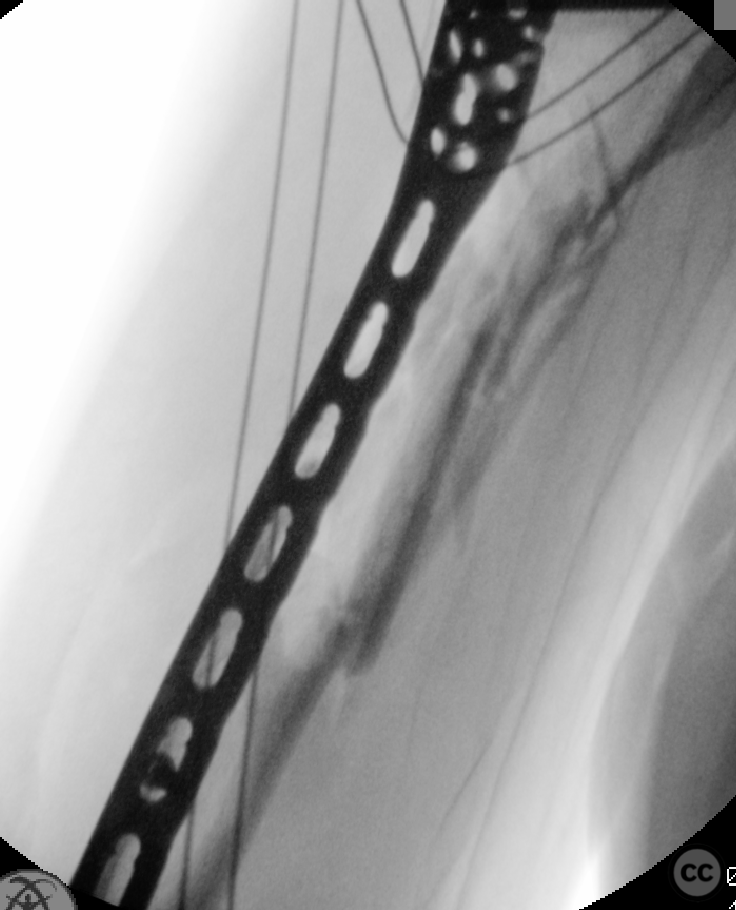
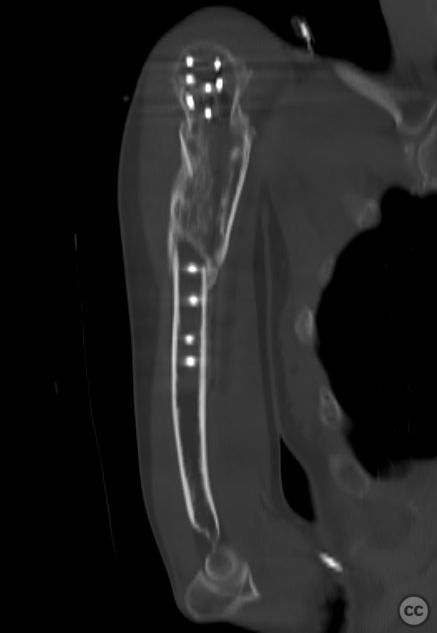
Anatomical surgical approach: A deltopectoral approach was utilized, involving the release of the subscapularis muscle to access the anterior aspect of the joint. This allowed for identification and partial reduction of the glenoid fracture. Despite incomplete reduction, sufficient stability of the glenohumeral joint was achieved. Percutaneous introduction of two 4.0mm cannulated screws under the acromion secured the superior glenoid rim to the scapular neck. For the humerus, an anterolateral plate position was selected without debridement of existing fracture callus/pannus, direct visualization, or manipulation of the fracture. Longitudinal alignment was facilitated by axial traction using a Spider Arm Positioner, and a long Philos plate was applied in a bridging construct.
Operative remarks:The surgical strategy accepted some rotational malreduction of the scapula fracture, prioritizing glenohumeral stability over complete anatomical reduction of the scapula.
Postoperative protocol: Postoperative rehabilitation protocol included active and passive range of motion exercises, with gradual increase in range of motion beyond 90 degrees and initiation of weight-bearing activities starting 6 weeks post-surgery.
Follow up: At 9 months follow-up, radiographic evaluation showed consolidation and remodeling of fractures with the patient reporting pain-free range of motion of approx 100deg flexion and abduction
Orthopaedic implants used: Orthopaedic implants used: Long Philos plate, 4.0mm cannulated screws.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1663 times
26 Mar 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Multifragmentary Proximal Humerus Fracture with Scapula Fracture in a Polytrauma Patient. Journal of Orthopaedic Surgery and Traumatology. Case Report 49325805 Published Online Mar 26 2024.