






Apple-bite posterolateral corner and ACL / Eminentia Avulsion
Score and Comment on this Case
Clinical Details
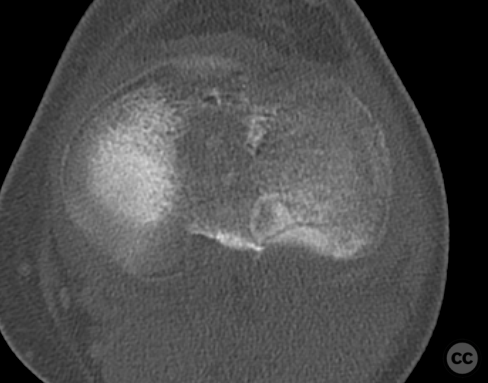
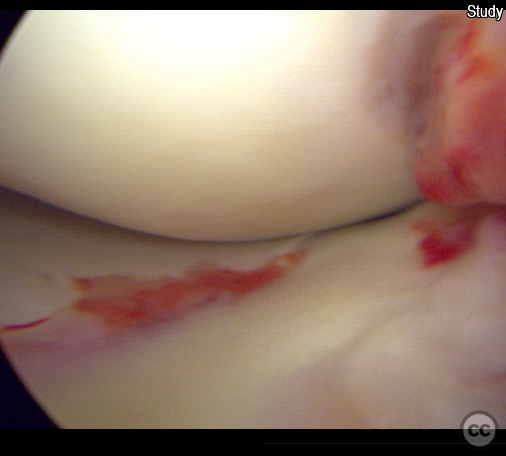
Clinical and radiological findings: A 36-year-old male presented one week after sustaining a knee injury during a football tackle. Examination revealed residual swelling and an unstable knee with a moderate pivot shift. CT imaging identified a posterolateral apple-bite tibial plateau fracture and an associated bony avulsion of the ACL. No MRI was performed as arthroscopy was anticipated and we address any potential meniscal injuries spontaneously
Preoperative Plan
Planning remarks: The surgical plan involved an arthroscopic-assisted approach for both the fracture reduction and the ACL avulsion fixation. The goals were to achieve anatomical reduction of the posterolateral tibial plateau fracture and secure fixation of the ACL avulsion using a minimally invasive technique. The anticipated approach for the fracture was a mini-open approach just inferior to Gerdy's tubercle, with arthroscopic assistance for visualization and guidance. For the ACL avulsion, an arthroscopic transosseous fibertape fixation technique was planned, utilizing an anterior cortical endobutton for fixation.
Surgical Discussion
Patient positioning: The patient was positioned supine
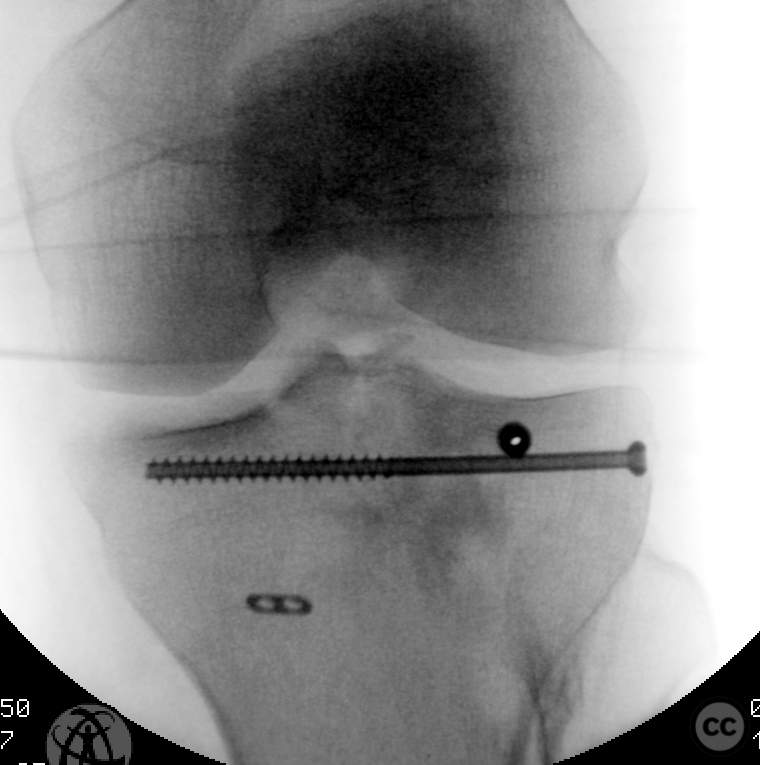
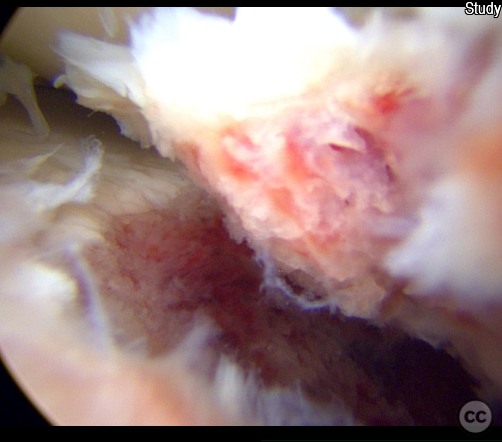
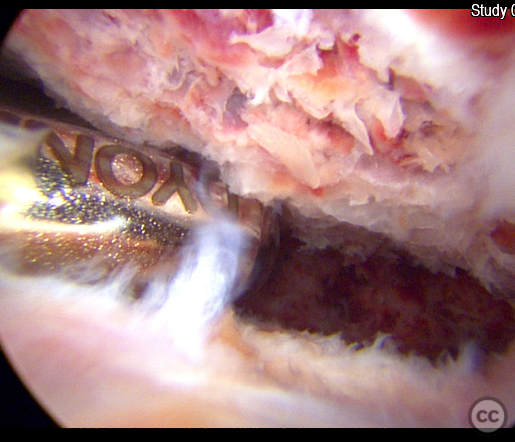
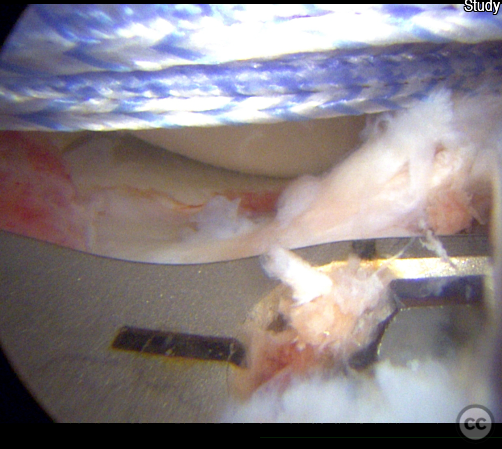
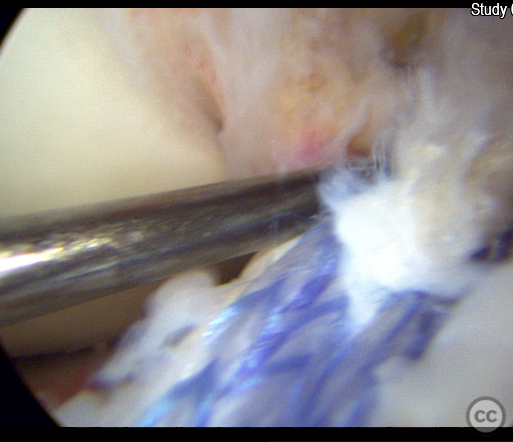
Operative remarks:A mini-invasive approach was made to the lateral tibial metaphysis, just inferior to Gerdy's tubercle. An 8mm osteotomy window was created for access. Under fluoroscopic and arthroscopic guidance, a bone tamp was used for reduction of the posterolateral corner fracture. Vitoss bone graft substitute was used to fill any defect voids. Subsequently, 4.0mm cannulated screws were used for 'jail-screw' fixation of the reduced fracture. For the ACL avulsion, an arthroscopic fibertape lasso suture technique was employed around the ACL stump, followed by retrograde drilling through the ACL footprint fragment. The fibertape was then shuttled anterograde to the anterior tibia, with tensioning of the suture and securing over an endobutton.
Postoperative protocol: Postoperatively, the patient was placed in a range of motion orthosis for 8 weeks to protect the repair while allowing gradual increase in knee ROM
Orthopaedic implants used: 4.0mm cannulated screws - Vitoss bone graft substitute - Arthrex Fibertape and cortical endobutton
PubMed® Literature Review
Generated by The Literature - Realtime PubMed® AnalysisArthroscopy-assisted reduction and fixation (ARIF) has emerged as an alternative technique aimed at minimizing soft tissue trauma while allowing for precise fracture reduction and treatment of concomitant intra-articular pathologies [2-4].
The use of ARIF in treating Schatzker I-III tibial plateau fractures has been supported by several studies demonstrating favorable clinical outcomes with minimal complications. Compagnoni et al. reported excellent Rasmussen scores and Visual Analog Scale (VAS) scores in four patients treated with ARIF at short-term follow-up [2]. Similarly, Chan highlighted the advantages of arthroscopy-assisted procedures over traditional open methods, including direct visualization for accurate fracture reduction and reduced morbidity [3].
Shamrock et al.'s matched cohort analysis comparing AATPFF against traditional fixation techniques revealed that AATPFF is associated with significantly lower rates of minor medical complications (8.2% vs 2.7%), major medical complications (9.9% vs 4.6%), surgical complications (13.2% vs 2.7%), and emergency department visits within 90 days post-surgery [4]. This suggests that ARIF not only maintains comparable efficacy in achieving anatomical reduction but also enhances patient safety by reducing postoperative complication risks.
However, despite these promising results, concerns remain regarding the potential limitations of ARIF, such as its technical demand and learning curve which might limit its widespread adoption [5]. Moreover, there's ongoing debate on whether it can achieve equivalent articular surface restoration compared to open reduction internal fixation (ORIF), especially in more complex or bicondylar fractures where optimal plate positioning is crucial for stability [1].
Le Baron et al.’s study provided a comparative analysis between ARIF and ORIF for Schatzker I-III fractures indicating no significant differences in clinical outcomes or radiological signs of osteoarthritis long term; however they noted that ARIF offered slightly better Hospital for Special Surgery (HSS) scores than ORIF did [6]. This reinforces the notion that while both techniques are viable options for managing selected tibial plateau fractures, surgeon expertise plays a critical role in determining the most appropriate approach.
Jiang et al.’s systematic review further supports this perspective by showing that compared to ORIF, ARIF leads to faster postoperative recovery better clinical function without compromising on radiological outcomes or increasing complication rates significantly [12].
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1664 times
05 Jul 2023
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2023). Apple-bite posterolateral corner and ACL / Eminentia Avulsion. Journal of Orthopaedic Surgery and Traumatology. Case Report 49528802 Published Online Jul 05 2023.