


Distal Tibial Salter-Harris IV with Distal Diaphyseal Fibula Fracture
Score and Comment on this Case
Clinical Details
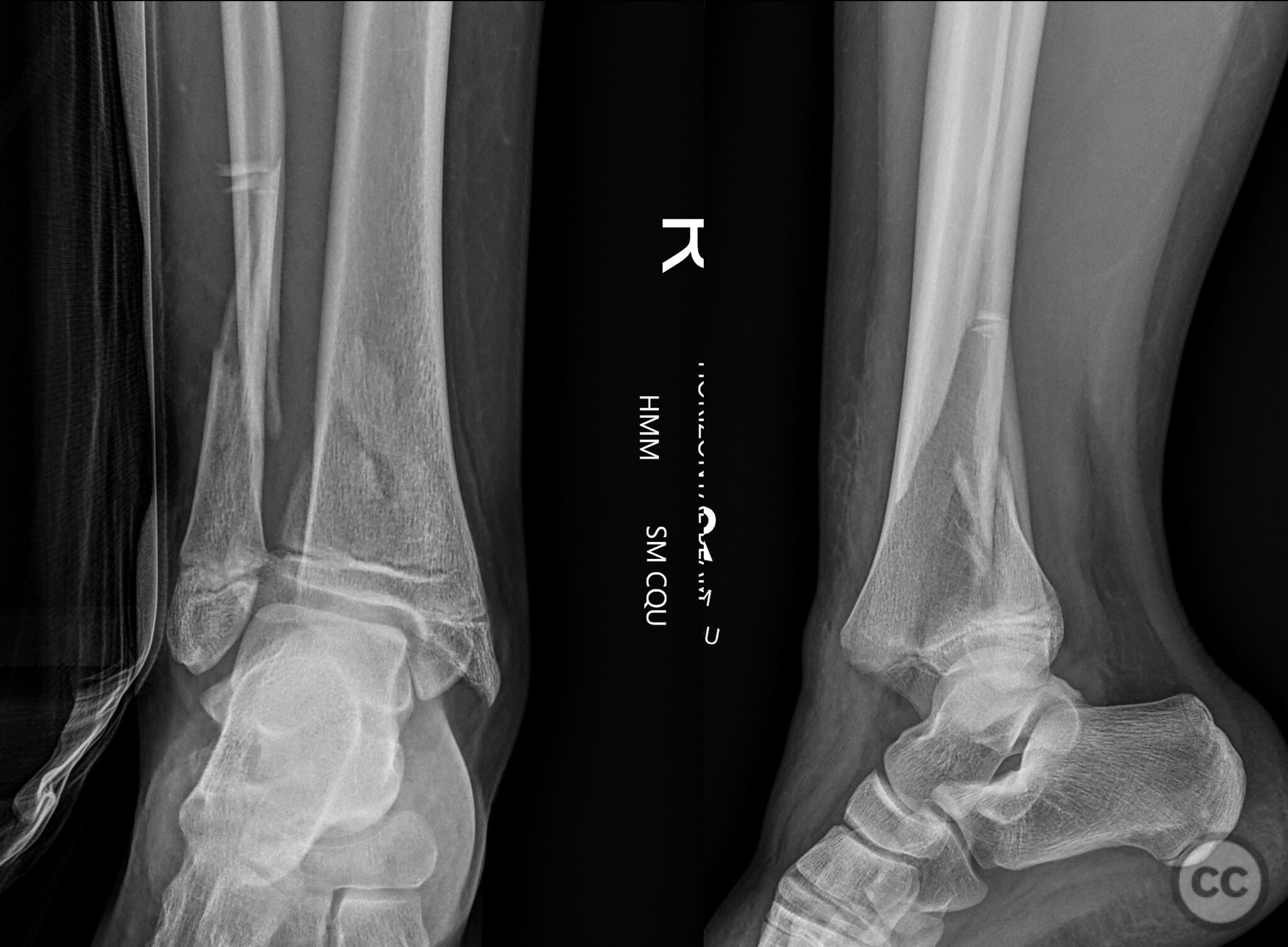
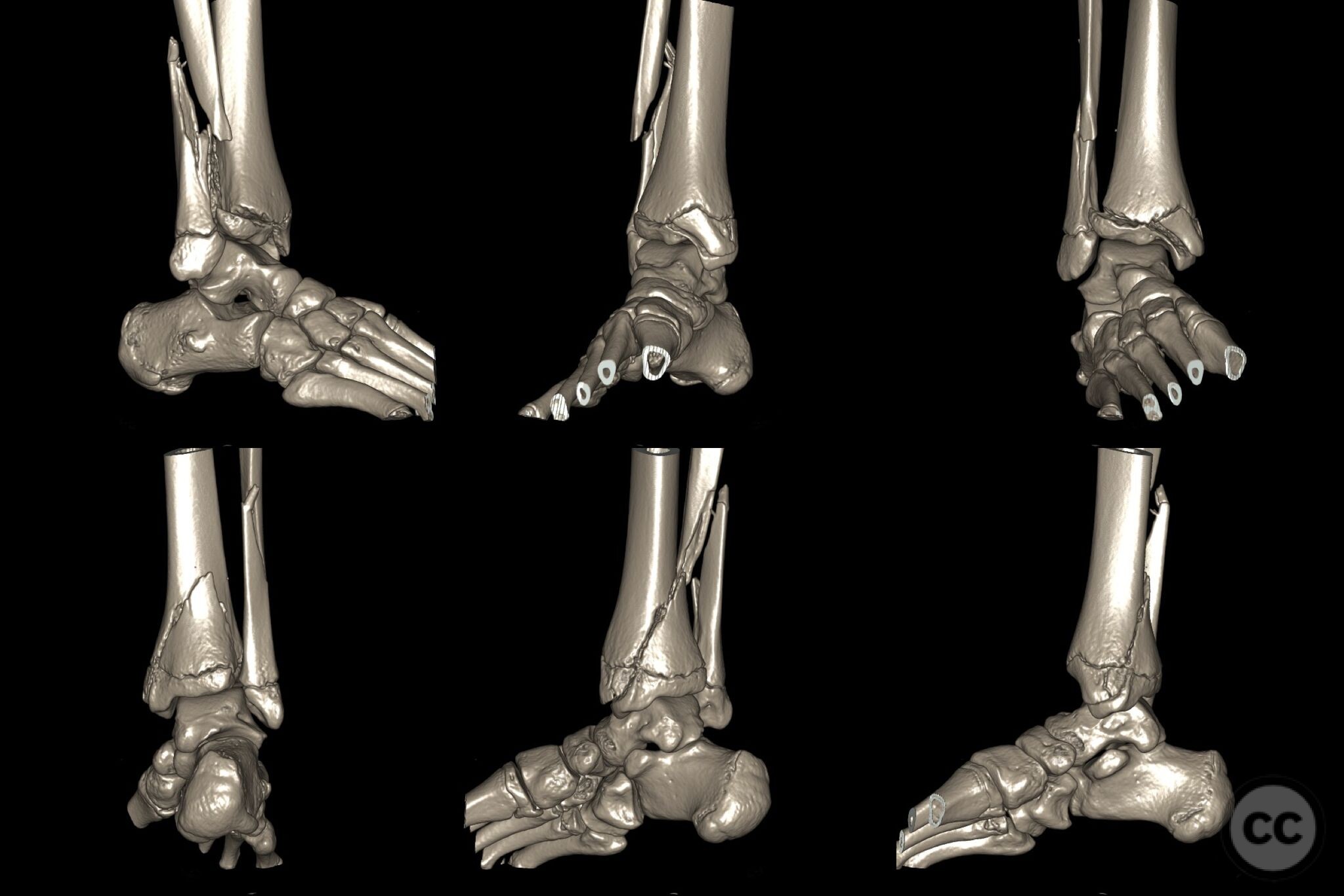
Clinical and radiological findings: A 14-year-old female presented following a fall from a makeshift swing, resulting in her leg being trapped underneath her. Initial clinical examination revealed a closed distal tibial fracture with a distal diaphyseal fibula fracture. Radiographs and subsequent CT imaging confirmed a Salter-Harris IV fracture of the distal tibia, behaving more like a Salter-Harris II fracture without extension into the ankle joint. The CT scan also identified entrapped loose fragments within the metaphyseal fracture line. Additionally, small avulsion fractures were noted at the base of the 1st and 2nd metatarsals, with subtle instability of the Lisfranc interval.
Preoperative Plan
Planning remarks: The preoperative plan involved a postero-lateral approach to retrieve the entrapped fragments and reduce the distal tibia, supplemented by an antero-medial approach for additional access and reduction. A postero-lateral pre-contoured plate was planned for fixation, with an additional antero-medial to postero-lateral lag screw in the epiphysis. Reduction of the fibula was deemed crucial for achieving proper alignment of the tibial fracture.
Surgical Discussion
Patient positioning: Not Specified
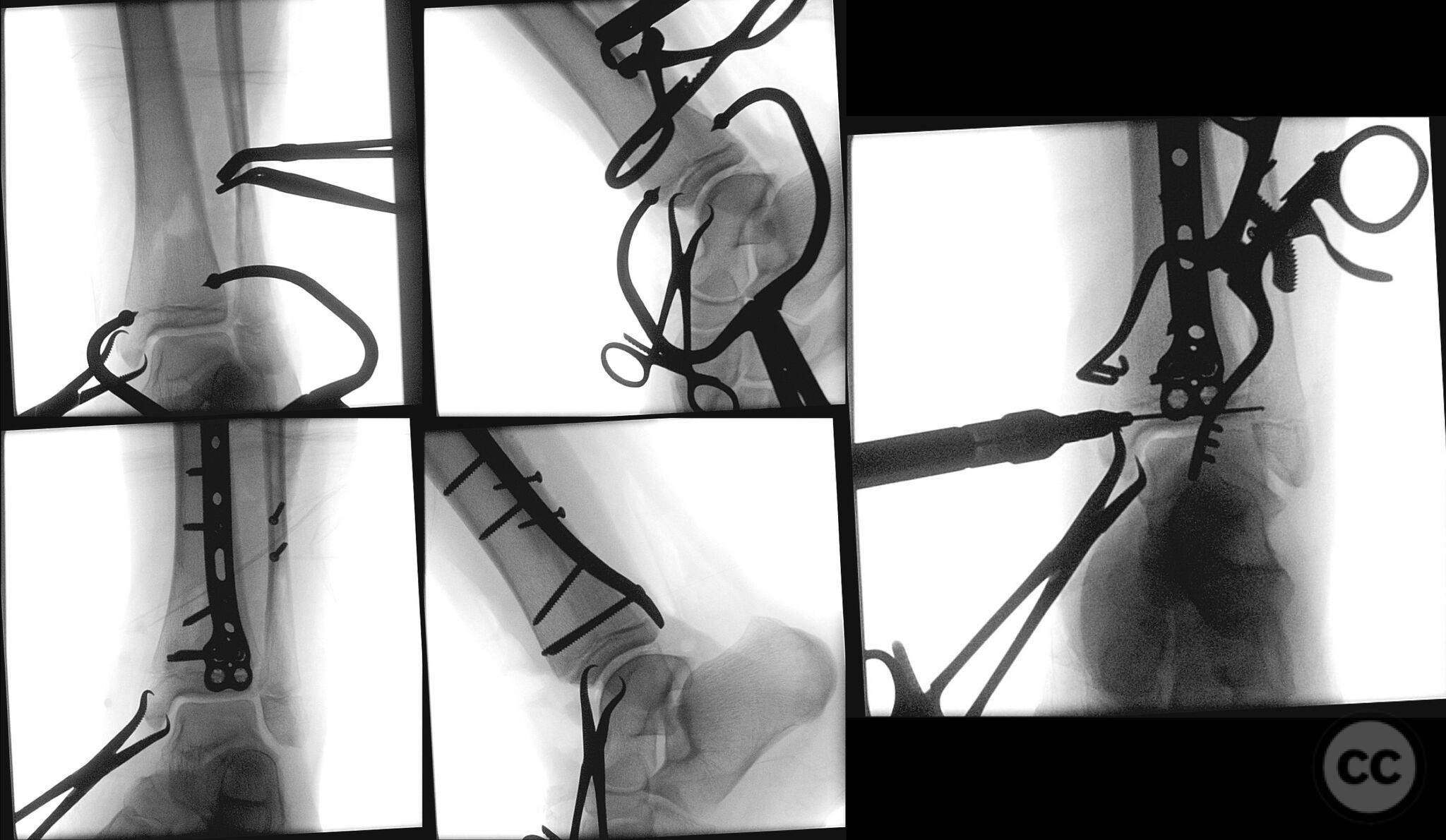
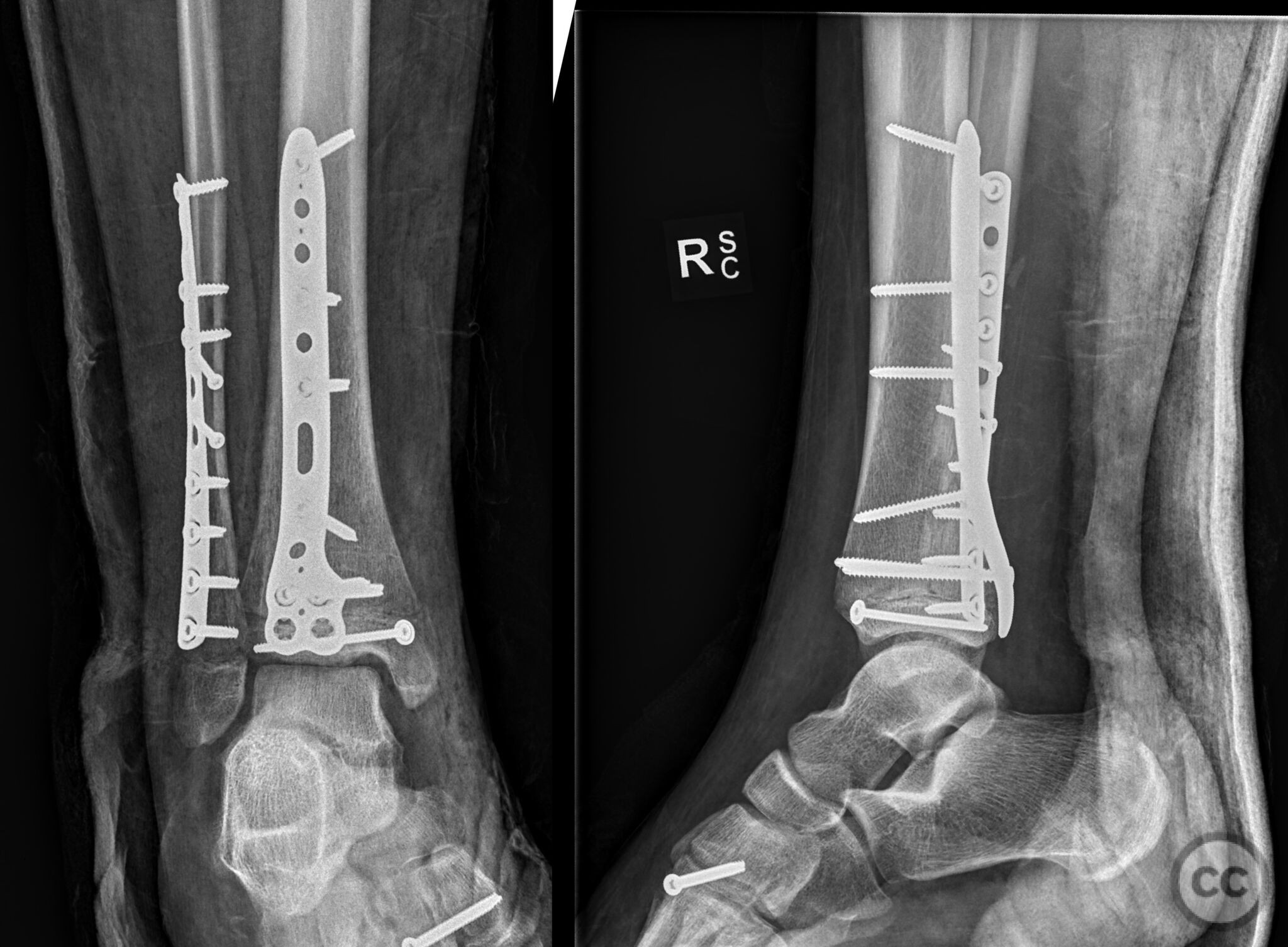
Anatomical surgical approach: The surgical approach commenced with a longitudinal incision along the postero-lateral aspect of the distal tibia, extending proximally to allow adequate exposure. The intermuscular septum was identified and retracted, followed by subperiosteal dissection to expose the fracture site. Entrapped fragments were retrieved, and reduction was achieved in stages. A supplementary antero-medial incision was made to assist in reduction and fixation. The distal tibia was stabilized using a pre-contoured postero-lateral plate, and an additional lag screw was placed from antero-medial to postero-lateral through the epiphysis.
Operative remarks:Intraoperatively, it was noted that fibula reduction played a key role in achieving satisfactory alignment of the tibial fracture. The presence of small avulsion fractures at the base of the 1st and 2nd metatarsals and subtle Lisfranc instability were addressed conservatively. The reduction was confirmed fluoroscopically, and fixation was deemed stable.
Postoperative protocol: I do find that the posterolateral approaches do end up fairly stiff if you don’t get them moving early so for me now they all go into CAM boots or equivalent early and start ankle and STJ ROM.
Follow up: Originally posted on LinkedIn by Simon Donald, Orthopaedic Surgeon, Bundaberg, Queensland, Australia
Orthopaedic implants used: Pre-contoured postero-lateral plate, antero-medial to postero-lateral lag screw
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 315 times
31 Jul 2024
Add to Bookmarks
Full Citation
Cite this article:
LinkedIn. (2024). Distal Tibial Salter-Harris IV with Distal Diaphyseal Fibula Fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 5374476 Published Online Jul 31 2024.