





Distal Radius Malunion Osteotomy with Volar Locking Plate
Score and Comment on this Case
Clinical Details
Clinical and radiological findings: An 18-year-old male presented with a distal radius fracture sustained 4 months prior, initially managed conservatively. The patient developed a malunion with severe dorsal displacement. Radiographs confirmed the malunion with significant dorsal angulation and displacement.
Preoperative Plan
Planning remarks: The preoperative plan included a corrective osteotomy of the distal radius using a volar locking plate. The approach was planned via a modified Henry approach to allow for optimal visualization and correction of the deformity.
Surgical Discussion
Patient positioning: The patient was positioned supine on the operating table, and a tourniquet was applied to the upper arm to achieve a bloodless field.
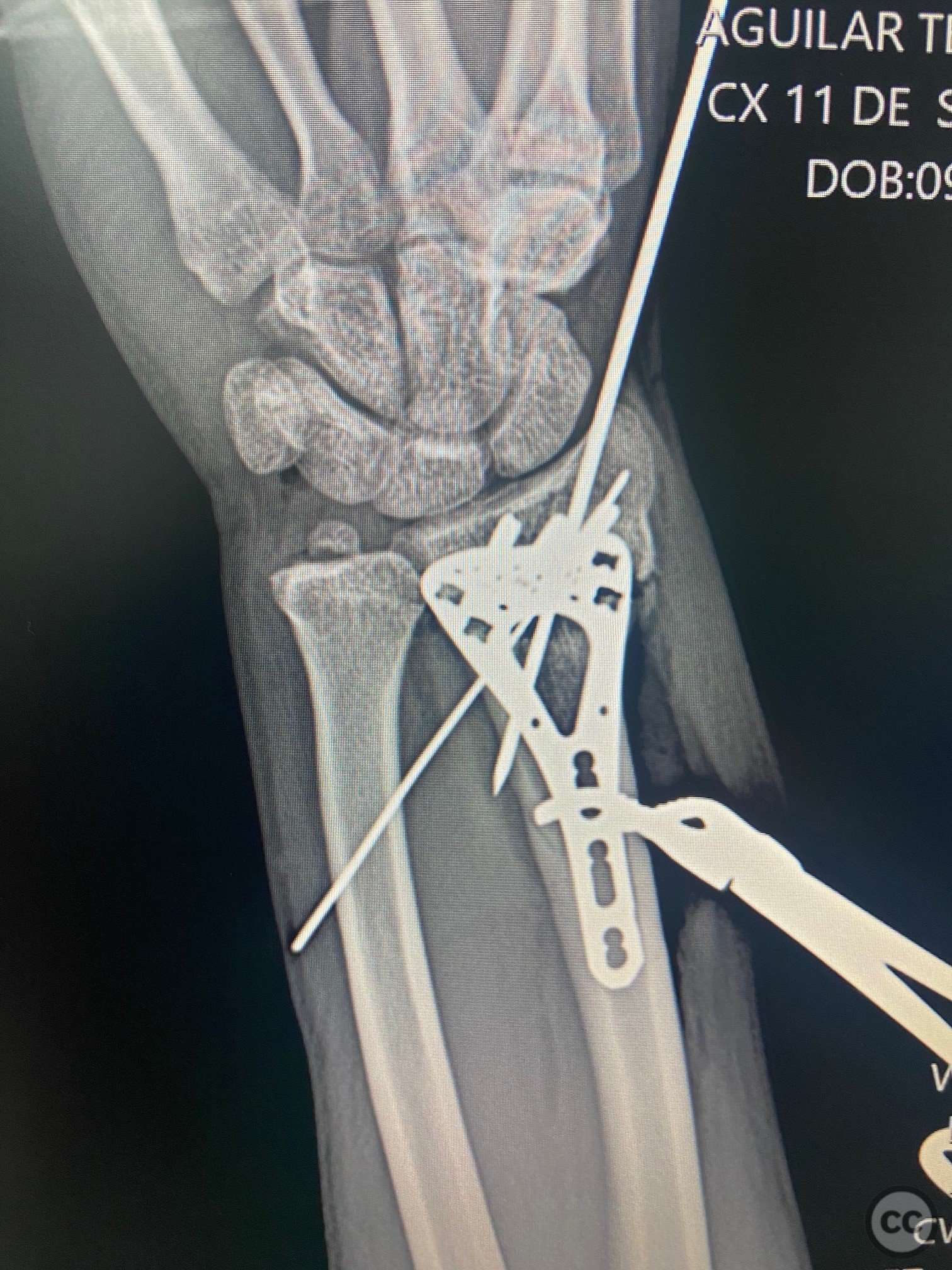
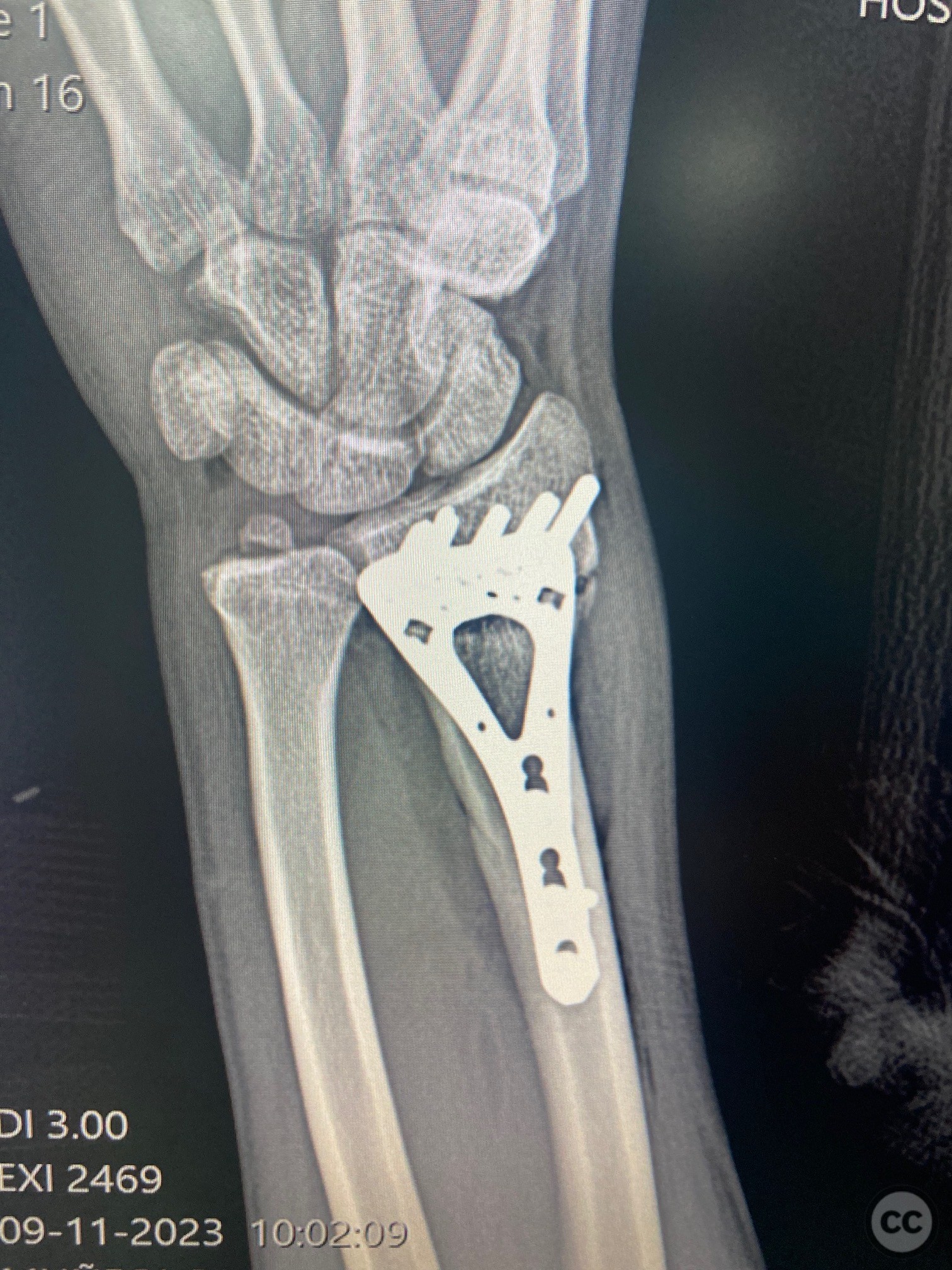
Anatomical surgical approach: A modified Henry approach was utilized, involving an incision along the flexor carpi radialis tendon. The flexor tendons were retracted ulnarly, and the radial artery was protected laterally. The pronator quadratus muscle was elevated subperiosteally to expose the distal radius. An anatomical volar distal radius plate was initially placed with two distal screws, ensuring parallel alignment to the joint in the lateral projection. A Kirschner wire was used as a guide for the osteotomy, which was performed in the metaphyseal region. The plate and screws were temporarily removed to complete the osteotomy. The plate was then repositioned with distal screws, and reduction forceps were applied to the radial diaphysis to correct the deformity. Temporary stability was achieved with two Kirschner wires, followed by final fixation with distal and proximal screws.
Operative remarks:Intraoperatively, radiographic verification confirmed appropriate alignment and fixation. A secondary dorsal approach was made to introduce autologous iliac crest bone graft into the osteotomy site to enhance healing.
Postoperative protocol: Postoperatively, the patient was advised to avoid weight-bearing activities on the affected wrist for 6 weeks. Gradual range of motion exercises were initiated at 2 weeks post-surgery, progressing to strengthening exercises at 6 weeks.
Follow up: Not specified
Orthopaedic implants used: Orthopaedic implants used: - Volar locking distal radius plate - Kirschner wires - Autologous iliac crest bone graft
Search for Related Literature


Industry Sponsership
contact us for advertising opportunities
Article viewed 295 times
01 Aug 2024
Add to Bookmarks
Full Citation
Cite this article:
LUIS LEONCIO TEMOCHE DIAZ. (2024). Distal Radius Malunion Osteotomy with Volar Locking Plate. Journal of Orthopaedic Surgery and Traumatology. Case Report 5691038 Published Online Aug 01 2024.