








Reduction of the radial column preserving Brachioradialis using a Hintermann k-wire retractor
Score and Comment on this Case
Clinical Details
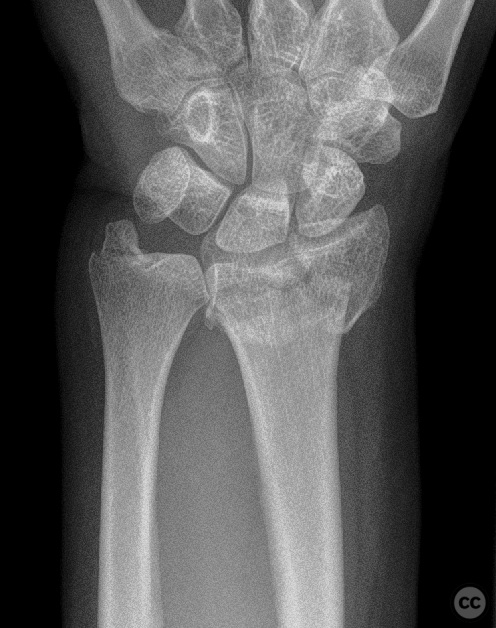
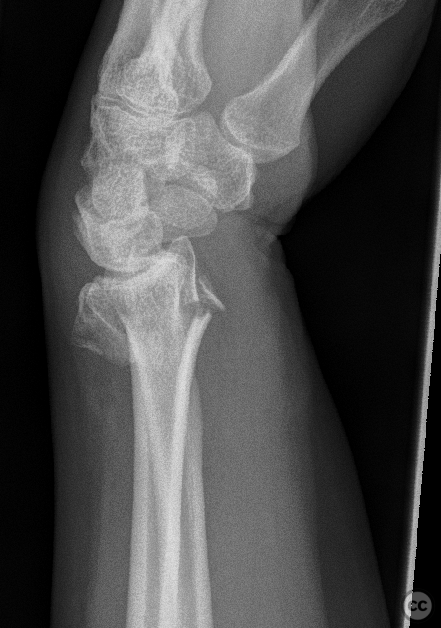
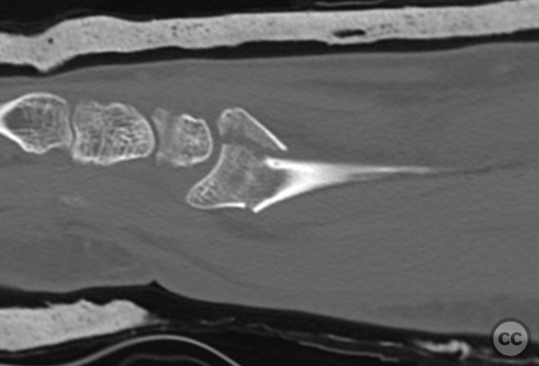
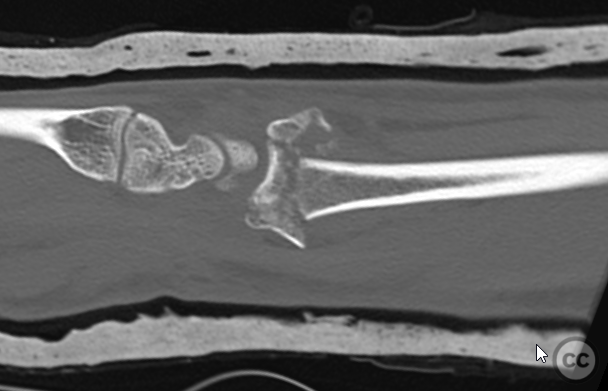
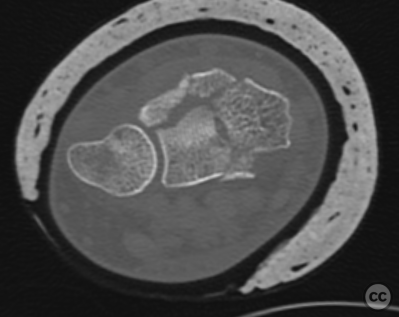
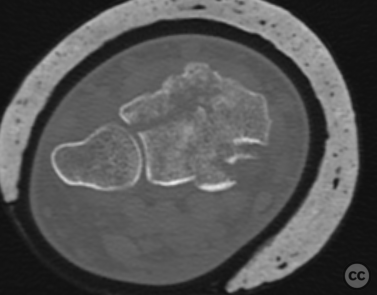
Clinical and radiological findings: A 56-year-old female patient experienced a ground-level fall during outdoor hiking activities, resulting in a dorsally angulated distal radius fracture. Preoperative computed tomography (CT) imaging revealed an intra-articular distal radius fracture characterized by a radial column fragment volarly displaced, a set fragment, two dorsal rim fragments including Lister's tubercle, and central impaction of the lunate fossa fragment. The brachioradialis muscle exerted a pulling force on the radial styloid fragment, contributing to its radial translation and proximal impaction.
Preoperative Plan
Planning remarks: The surgical plan involved a Henry's approach to the distal radius. The strategy aimed to counteract the pull of the brachioradialis on the radial styloid fragment using K-wires and a Hintermann distractor for restoration of radial inclination, length, and correction of radial translation.
Surgical Discussion
Patient positioning: The patient was positioned supine with the arm extended and supported on a hand table
Anatomical surgical approach: A Henry's approach was utilized, extending distally in a zigzag fashion to allow for adequate exposure of the distal radius fragments. This approach facilitated direct visualization and manipulation of the fracture components.
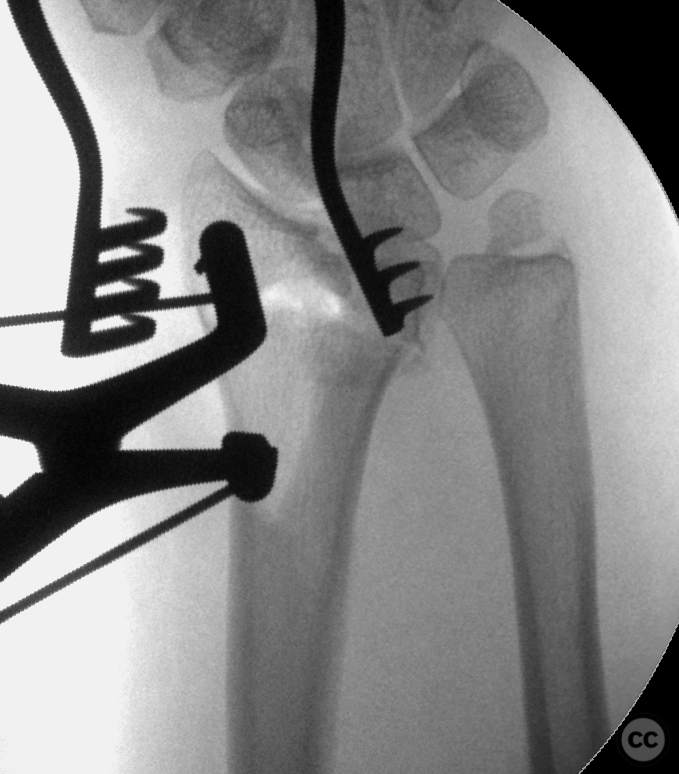
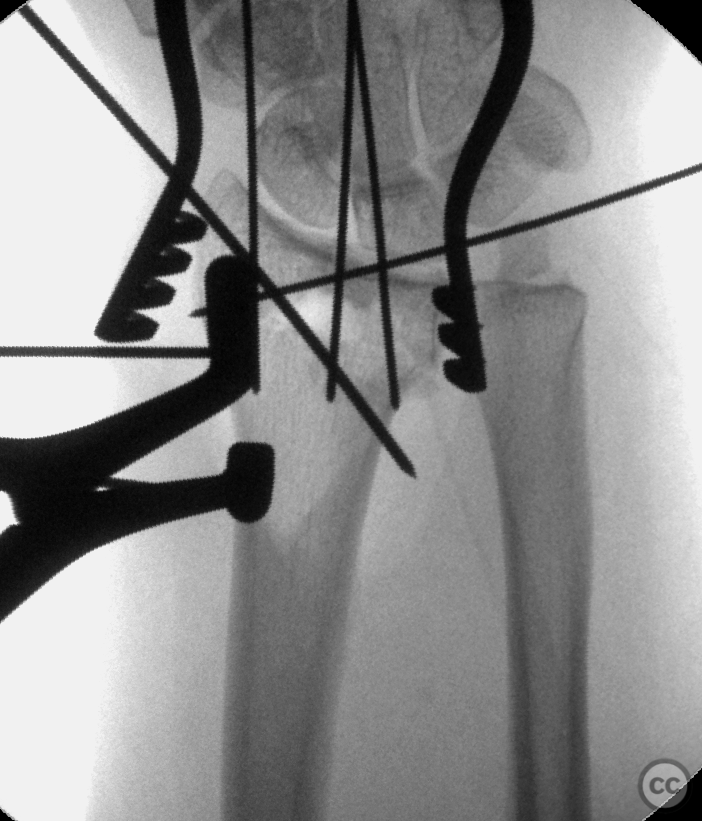
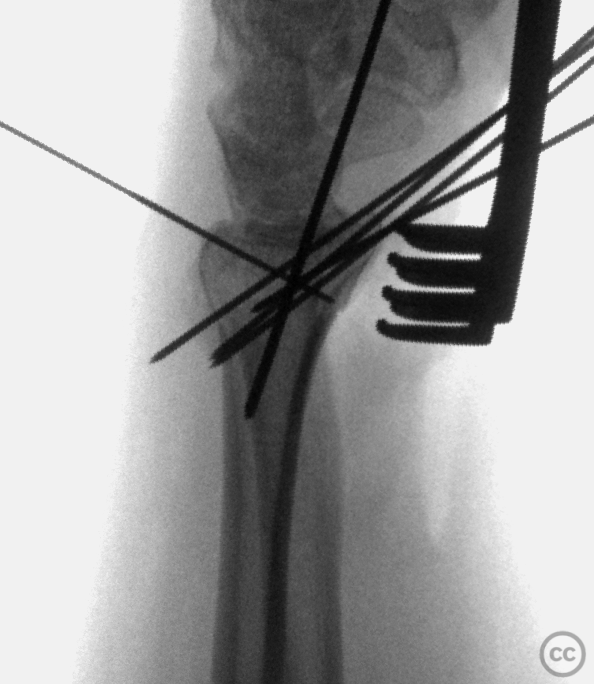
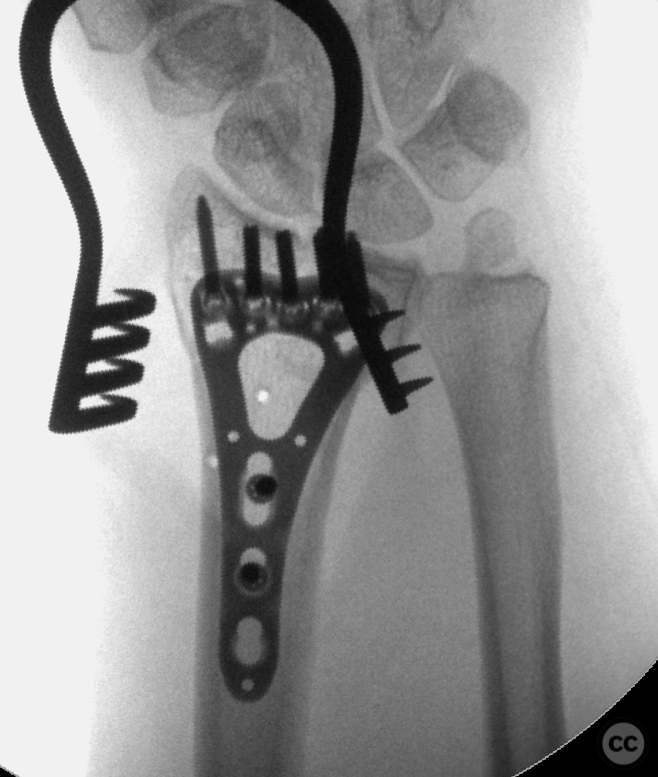
Operative remarks:Initially, 1.2 or 1.6 mm K-wires were inserted proximally and distally into the fracture at the radial styloid. A Hintermann K-wire distractor was employed to achieve radial inclination, length, and correction of radial translation, secured with a 1.6 mm trans-styloid K-wire. The lunate fossa fragment was addressed through a cortical window on the proximal volar metaphysis using a small bone tamp for reduction, followed by fixation with a 1.2 mm K-wire. Dorsal ulnar fragments and Lister's tubercle were percutaneously pinned from the dorsal aspect with 1.0 mm K-wires. A distal-fragment-first technique was used to resolve residual dorsal inclination, with plate fixation initiated distally using five subchondral screws, then dynamically reducing the proximal plate to the radial diaphysis to correct volar tilt and fine-tune residual radial translation adjustments.
Postoperative protocol: Immediate postoperative mobilization; active finger motion encouraged from day one. Gradual wrist mobilization initiated at 2 weeks postoperatively under physiotherapist guidance, progressing to full weight-bearing as tolerated by 6 weeks.
Follow up: Not specified.
Orthopaedic implants used: Not specified.
PubMed® Literature Review
Generated by The Literature - Realtime PubMed® AnalysisThe management of distal radius fractures, particularly AO type C fractures, often involves complex decision-making regarding the approach to reduction and fixation. One aspect that has garnered attention is the role of brachioradialis (BR) release or tenotomy in facilitating these procedures without compromising wrist and elbow function postoperatively.
Ma et al. [1] conducted a prospective comparative study examining whether BR release during volar plate fixation for type C distal radius fractures eases internal reduction and fixation without adversely affecting wrist or elbow function. Their findings suggest that BR release significantly shortens the time required for reduction and internal fixation while not impacting functional outcomes negatively when assessed using various scoring systems such as MEPS, DASH, G-W, PRWE, VAS scores, and radiological parameters at both 6 and 12 months postoperatively.
Similarly, Kim et al. [2] investigated whether BR release affects elbow flexion strength and wrist function following volar plate fixation for unstable distal radius fractures. Their results indicated no significant differences in elbow flexion strength/endurance or secondary outcome variables like grip strength, pain levels (VAS score), DASH score, or radiographic parameters between patients with preserved versus released BR.
Hohendorff et al. [3] described a surgical technique involving repair of the pronator quadratus muscle with part of the brachioradialis muscle insertion during volar plate fixation for distal radius fracture repair. This method aims to provide stable coverage over the volar locking plate by slight distal transposition to protect finger flexor tendons against irritation/rupture post-surgery.
Protopsaltis & Ruch [4] highlighted critical elements in utilizing a volar approach for distal radius fracture treatment including releasing the brachioradialis among other steps to gain adequate exposure necessary for optimal intra-articular reconstruction especially with advancements in locking plate technology expanding indications beyond simple displaced fractures.
Collectively these studies underscore that BR release during volar plating does not detrimentally affect long-term wrist or elbow functionality despite initial concerns regarding potential loss of strength or mobility due to tendon detachment [1-4]. Moreover, techniques incorporating parts of BR into repairs may offer additional benefits concerning soft tissue coverage over implants thereby potentially reducing complications related to tendon irritation/rubbing against hardware [3].
In conclusion, current literature supports that brachioradialis release can facilitate surgical procedures involved in fixing certain types of distal radius fractures without impairing functional outcomes related to wrist motion/strength or elbow flexibility/strength postoperatively. Such findings are crucial as they help refine operative strategies ensuring better patient recovery trajectories while minimizing risks associated with procedural complexities inherent in managing these common yet challenging injuries.
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1429 times
17 Apr 2024
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2024). Reduction of the radial column preserving Brachioradialis using a Hintermann k-wire retractor. Journal of Orthopaedic Surgery and Traumatology. Case Report 6075364 Published Online Apr 17 2024.