



Comminuted C2 articular distal humerus fracture without osteotomy
Score and Comment on this Case
Clinical Details
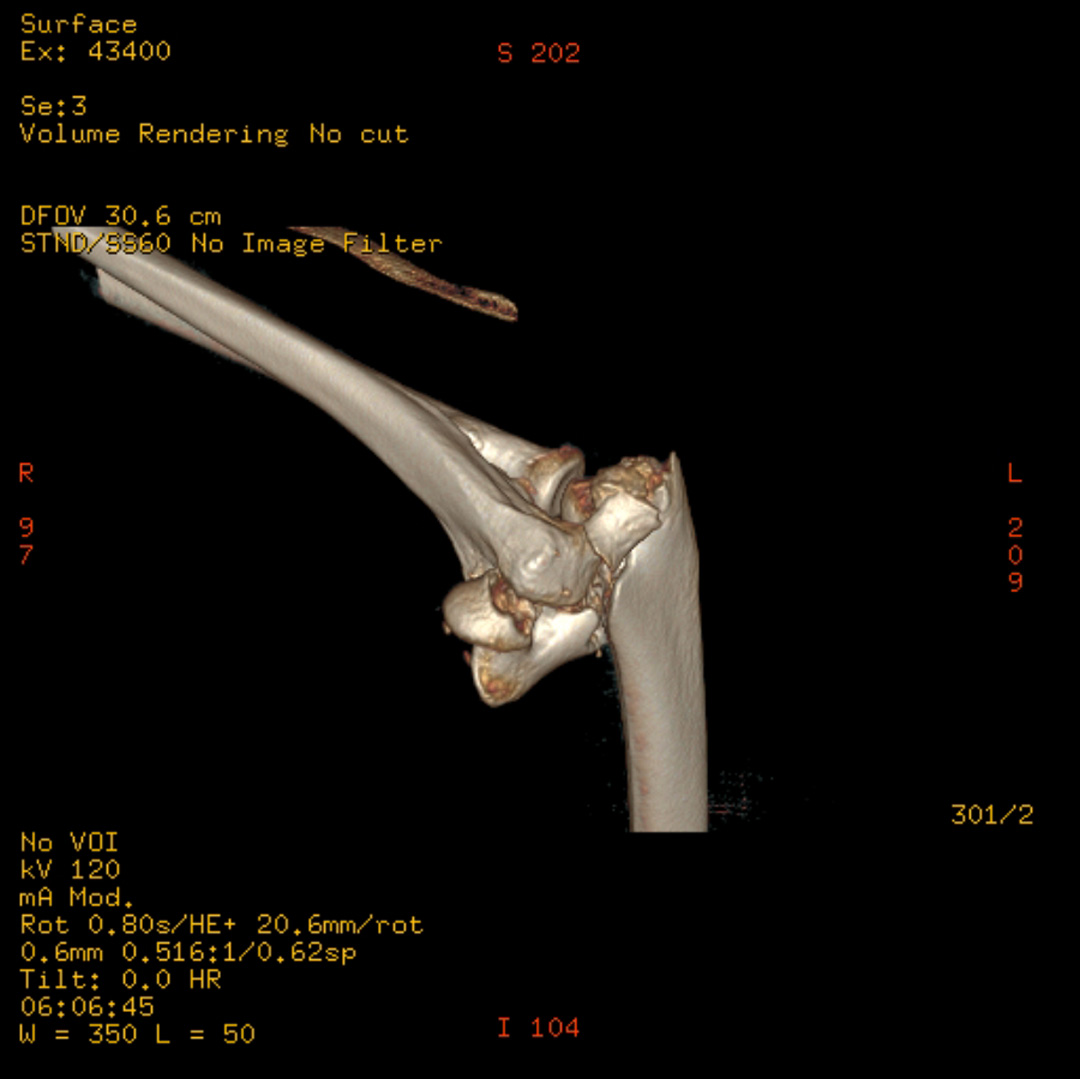
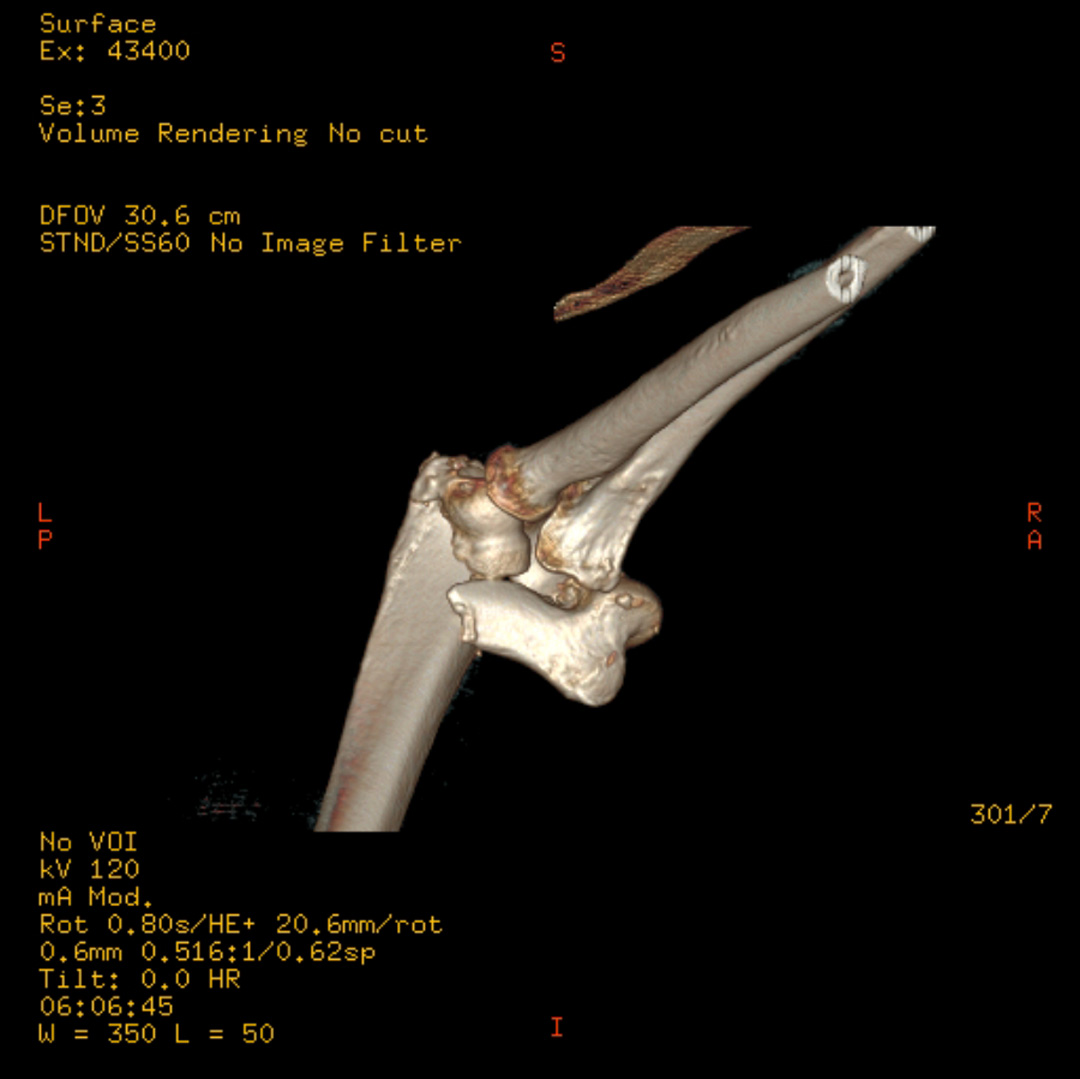
Clinical and radiological findings: This case is a 78-year-old male following a trip and fall onto the left forearm where he sustained a comminuted intra-articular fracture of the left distal humerus. Plain film and CT imaging demonstrated a sagittally split trochlea with an ulnar sided wedge/split component which had displaced ventrally and proximally. With it subluxation of the joint could be seen. More radially is a comminuted fracture of the remaining trochlea and capitellum. Not clearly appreciated in the imaging is an avulsion of the radial epicondyle. This was demonstrated intraoperatively to be a independent fragment. The operation was done prone with the arm positioned over a small side attachment allowing elbow flexion of over 90°. A simple dorsal approach with a radial curve around the olecranon was utilized. Given the size of the ulnar fragment I thought an olecranon osteotomy could be avoided in this case. After a neurolysis of the nerve we developed medial and lateral windows and then debrided the dorsal joint capsule. The ulnar fragment was able to be reduced anatomically with little difficulty. This allowed a solid basis for reconstruction of the residual joint surface from ulnar to radial. Due to poor bone stock of the comminuted radial fragments we opted for a fragment specific fixation using Arthrex 2.0 mm PLLA Trim It drill pins (re-absorbable K wires) along with 2 HBS midi PA screws to reconstruct the articular surface piece by piece. Following the reconstruction of the joint surface we placed dorsalradial and medioulnar distal humerus locking plates in 90° plating technique. The coronal screws from both plates in combination with the sub chondral transverse PLLA K wires produced a satisfyingly stable fixation of the articular components.
Preoperative Plan
Planning remarks:
Surgical Discussion
Operative remarks:Initially I believed that reduction of the ulnar fragment would provide an adequate anchor for reconstruction of the medial comminuted articular fragments as these would not be particularly hidden by the olecranon articular surface. Unfortunately the poor bone stock and comminuted nature of these fragments generated a frustrating situation of a lack of access and ability to create a stable definitive fixation. Perhaps stubbornly I stuck with my original plan of not doing an osteotomy, and whilst ultimately successful this did help push the operative time out to around three or four hours. Also the fixation of the discrete medial epicondyle avulsion was challenging. This fragment could not be captured by the radial plate/screws. In this otherwise comminuted region fragment to fragment fixation was not stable enough for the flexor origin. Ultimately we achieved fixation using a tension band construct utilizing the PLLA K wires and reabsorbable suture anchored to the plate.
Orthopaedic implants used: DePuy Synthes VA-LCP Distal Humerus Plates 2.7/35mm. Arthrex 2.0mm PLLA 'Trim-it' drill pins
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1823 times
15 Mar 2021
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2021). Comminuted C2 articular distal humerus fracture without osteotomy. Journal of Orthopaedic Surgery and Traumatology. Case Report 6570182 Published Online Mar 15 2021.