





Atypical ischial T acetabulum fracture
Score and Comment on this Case
Clinical Details
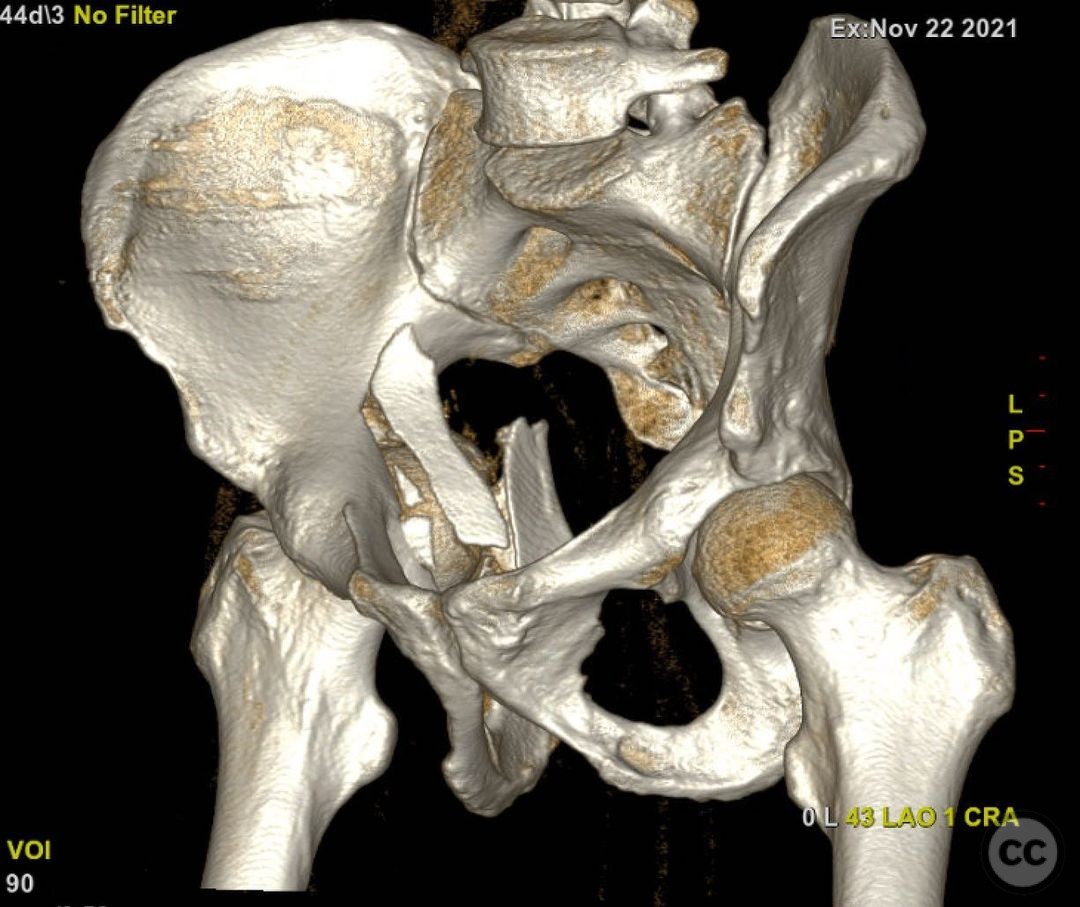
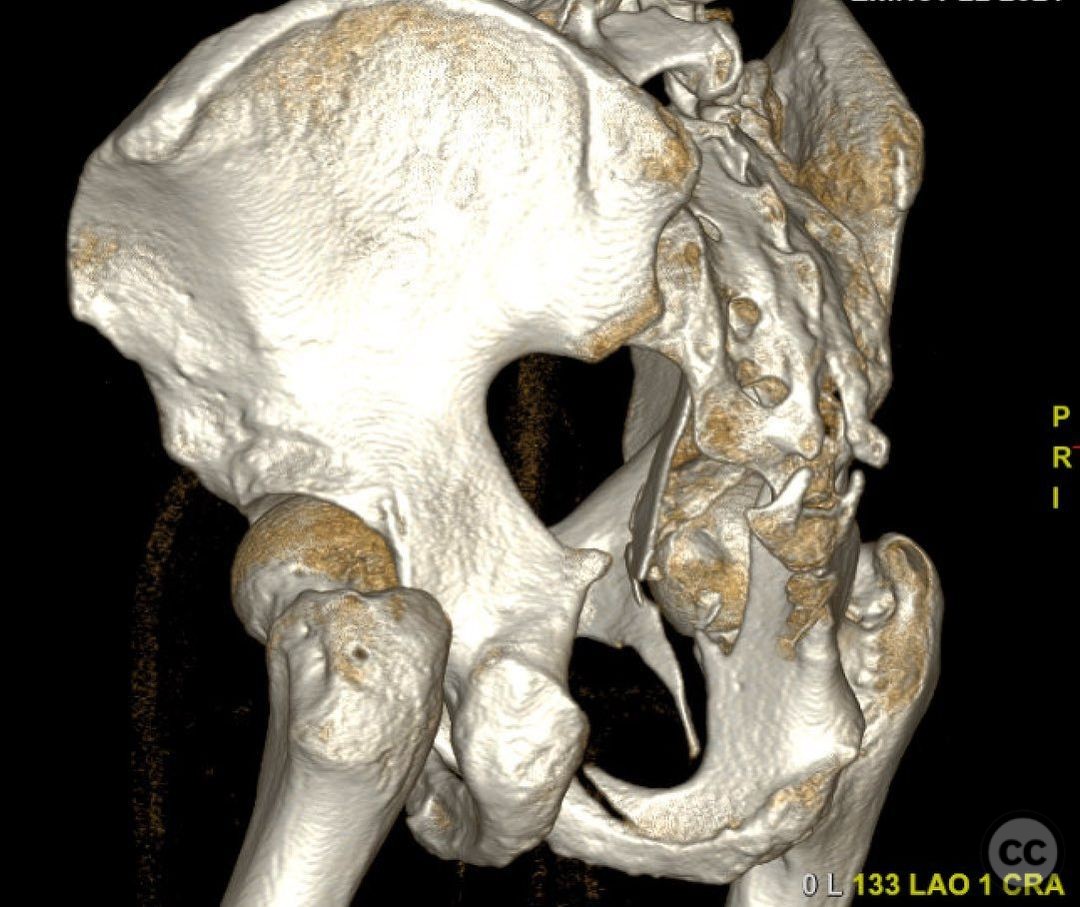
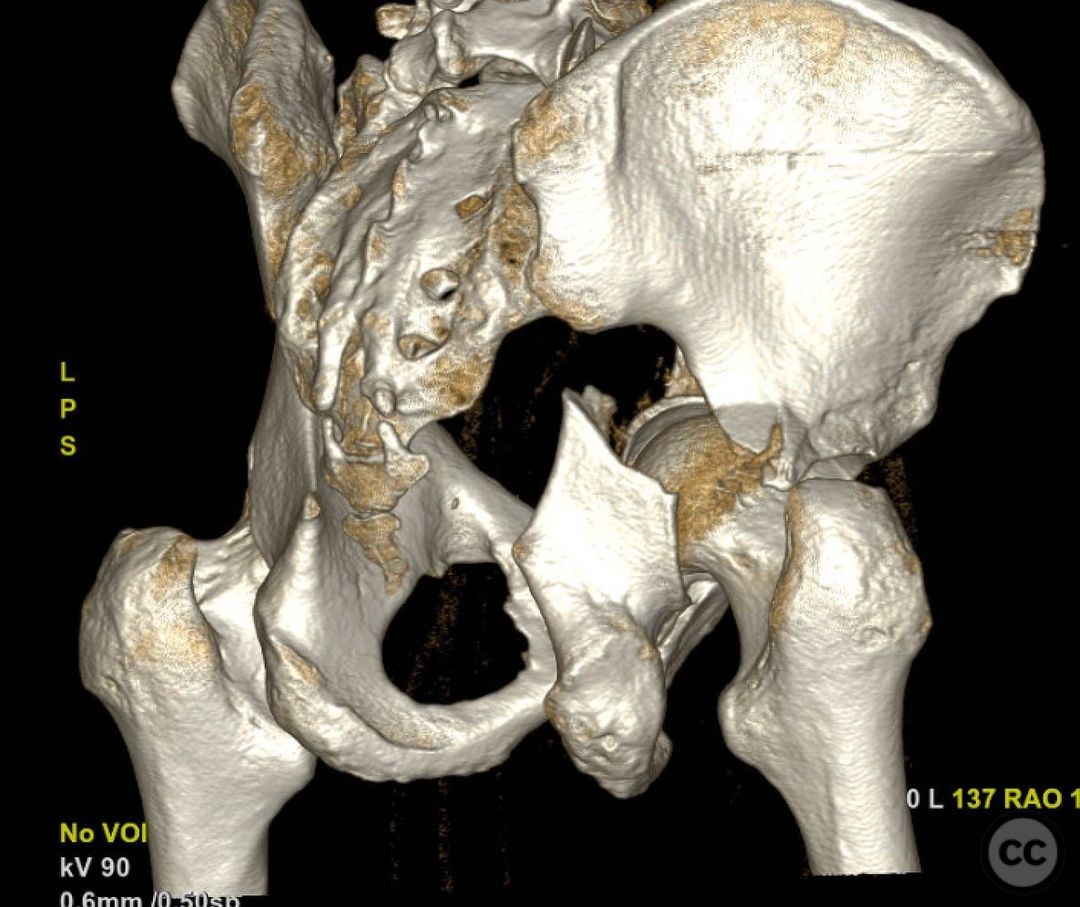
Clinical and radiological findings: 44yo male, high speed MVC. This is a rather unusual pattern which makes the planning, execution of approach(es), sequence, and reduction strategies fun and challenging. This tried oh so hard to be an ischial T, but the anterior column didn’t complete- leaving this is a variation. In spirit, this is a posterior column posterior wall variant. The purist will want to call it an incomplete ischial T. More importantly though is 1) the magnitude of posterior column displacement 2) posterior dislocation 3) the gigantic medialized free articular fragment (definitely the most interesting and challenging part of this case) and 4) posterior superior impaction.
Preoperative Plan
Planning remarks:
Surgical Discussion
Operative remarks:If it weren’t for this pesky medial dome fragment, this would be simple- KL approach, disimpact the joint, reduce, squeeze and plate the posterior column. But that medial joint piece is big and important. So it’s a game changer- here is how I thought about it and why we did what we did. Question to myself #1) can I reliably do this all from the back? Honest answer to myself- maybe but I’m not sure I have a good enough window thru the pc (very small pw fragments) so the main articular fragment (unclear if it’s free from its cortex or still intact to it. ) If I can’t get it right, can I fix the column/impaction/wall first and then go supine to get the fragment thru and AIP? Maybe, but if the column isn’t right, there’s no way I’ll get that large fragment right. Question #2) Can I do this all from the front? No. PC way off and low enough that getting it right from the front would be really hard- also, can’t directly reduce the impaction. Interestingly I asked a few of my acetabulum expert colleagues and they all had differing opinions! I decided to keep it as simple as possible- AIP to reduce the main joint fragment, then flip prone, KL, deal with the impaction and column. Unfortunately- that big joint fragment was free from its cortex, so what I was hoping was a really nice indirect read for the joint wasn’t helpful. In the end, minor articular malreduction.
Search for Related Literature

orthopaedic_trauma
- United States , Seattle
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 610 times
15 Jan 2023
Add to Bookmarks
Full Citation
Cite this article:
Surname, Initial. (2023). Atypical ischial T acetabulum fracture. Journal of Orthopaedic Surgery and Traumatology. Case Report 6996653 Published Online Jan 15 2023.