



Galeazzi fracture following radius atrophic non union
Score and Comment on this Case
Clinical Details
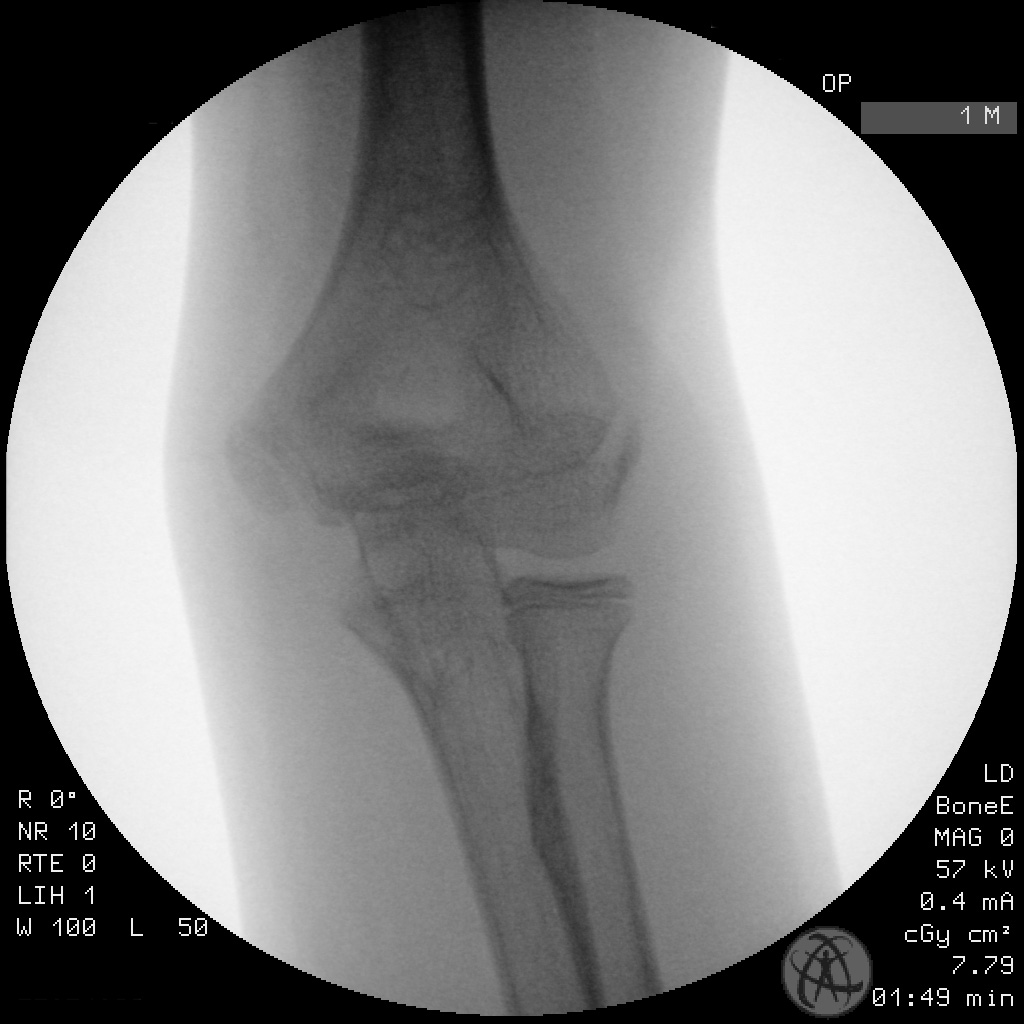
Clinical and radiological findings: This is an interesting case of a 12-year-old boy who sustained a Galeazzi fracture dislocation of the left distal radial diaphysis und DRUJ. The fracture as it presented to the emergency department was sustained with relatively a little force (the patient had pushed himself up from a chair). This occurred some six weeks following a supposed to greenstick fracture of the distal radius which was managed conservatively in a below elbow cost for two weeks. Sadly previous imaging was not available for review at the time of this presentation however we can appreciate on the primary imaging only very minimal callous development in the region of the original fracture (perhaps radially one might suggest a half millimeter callous layer). Otherwise of more significance is the relative radio-opaque/sclerotic looking bone immediately distal to the fracture. Given the relatively atraumatic circumstances of the current injury I assumed that we were dealing with refracture of an atrophic nonunion of the previous break which had now resulted in a complete Galeazzi fracture dislocation. Consent was obtained for a closed reduction and ECMES as well as open reduction and plate fixation . A limited initial attempt at closed reduction and intramedullary nail was entirely unsuccessful. The fracture could be passed with some force through the scleroticly closed region of the distal diaphysis however an anatomical reduction was not possible. Secondly the stability of the intramedullary device was inadequate to reduce and stabilize the DRUJ. The intramedullary nail was swiftly aborted and instead we opted for open reduction and internal fixation with a 2.7 mm LCP plate. The operation was done with the patient supine and the arm positioned on a small arm table affixed to the operating table. A volar Henry's approach to the distal radius was used. The fracture was located primarily under the origin of flexor pollicis longus. A limited release of flexor pollicis was necessary to completely expose the fracture. On examination of the fracture ends these demonstrated a scleriotic cortical rounding. The canal of the distal diaphyseal fragment was nearly completely obliterated with sclerotic bony change. After debridement of the sclerotic bone we positioned a LCP 2.7 mm plate using eccentric drilling and dynamic plate compression. Once the radius was anatomically reduced and fixed the DRUJ had spontaneously reduced and dynamic fluroscopy failed to demonstrate any further dynamic instability. We did not transfix the DRUJ, but chose to protect the reduction with postoperative immobilisation in an above elbow cast with the forearm in supination.
Preoperative Plan
Planning remarks:
Surgical Discussion
Operative remarks:This case was initially seen by one of the surgical trainees of the department, and had been significantly underestimated. The role of the nonunion was not appreciated initially, nor its impact on choise of fixation hardware. The complication of the concominant Galeazzi fracture dislocation (and the necessity to acheive a stable anatomical reduction to reduce the distal radioulnar joint) was similarly underappreciated. Ultimately a LCP plate With dynamic plate compression following fracture debridement was necessary to anatomically reduce both fracture and the dislocation. Some have commented that I should have transfixed the DRUJ, but given the radiologic stability we demonstrated after reduction, i think it was safe not to.
Orthopaedic implants used: DePuy Synthes Small Fragment LCP Plate 2.7
Author's Resources & References
Search for Related Literature

Dr Ed Oates
- Germany , Schleswig Holstein
- Area of Specialty - General Trauma
- Position - Specialist Consultant

Industry Sponsership
contact us for advertising opportunities
Article viewed 1144 times
15 Mar 2021
Add to Bookmarks
Full Citation
Cite this article:
Oates, E.J. (2021). Galeazzi fracture following radius atrophic non union. Journal of Orthopaedic Surgery and Traumatology. Case Report 7622379 Published Online Mar 15 2021.